The first widely used migraine-specific treatments, the triptans, were introduced in the early 1990s. These drugs marked a turning point towards more targeted management of migraine. However, a substantial proportion (around one third) of individuals do not respond adequately to current treatments. Many drugs primarily target head pain, despite non-pain symptoms like fatigue, light sensitivity and nausea often being just as debilitating. As a result, researchers continue to search for new drug targets. But how does a new migraine treatment turn from an idea into something prescribed in a clinic? This blog will give you some insights into what happens ‘behind the scenes’ of drug discovery.
Where do new ideas come from?
New treatment ideas begin with discovery science. As research improves what we know about what’s happening in the brain during a migraine attack, scientists identify biological processes that could be targeted with drugs. For example, Calcitonin Gene-Related Peptide (CGRP) was discovered to play a key role in migraine pain-signalling as its levels were shown to increase in people during attacks. This initial insight led to the development of therapies to block its effects, with some drugs now available. But not all scientific discoveries lead to the development of new drugs. Sometimes researchers can repurpose existing treatments, like botox, instead. In other cases, observing the strengths and weaknesses of existing drugs, helps researchers design safer or more effective options. New treatments rarely emerge in isolation but instead build on decades of accumulated research and clinical observations.
From the research lab:
Once an idea is generated, the earliest stage of drug development happens in laboratories. Scientists will first test compounds in preclinical models, like cells, animals or computer simulations, to look for signs that one of these compounds might improve migraine-related biology. You can think of drug discovery as testing many different keys in a complex lock (which may itself not yet be understood). If a particular compound is successful at improving migraine-related biology, it becomes a potential new medicine, known as a ‘drug candidate’. However, scientists may need to test thousands of compounds before finding one promising drug candidate, making this a challenging and time-consuming process. These initial investigations done in preclinical models allow researchers to begin to assess both how effective a drug candidate is at modifying migraine-related biology and whether it appears safe enough to progress further.
To the medicine cabinet:
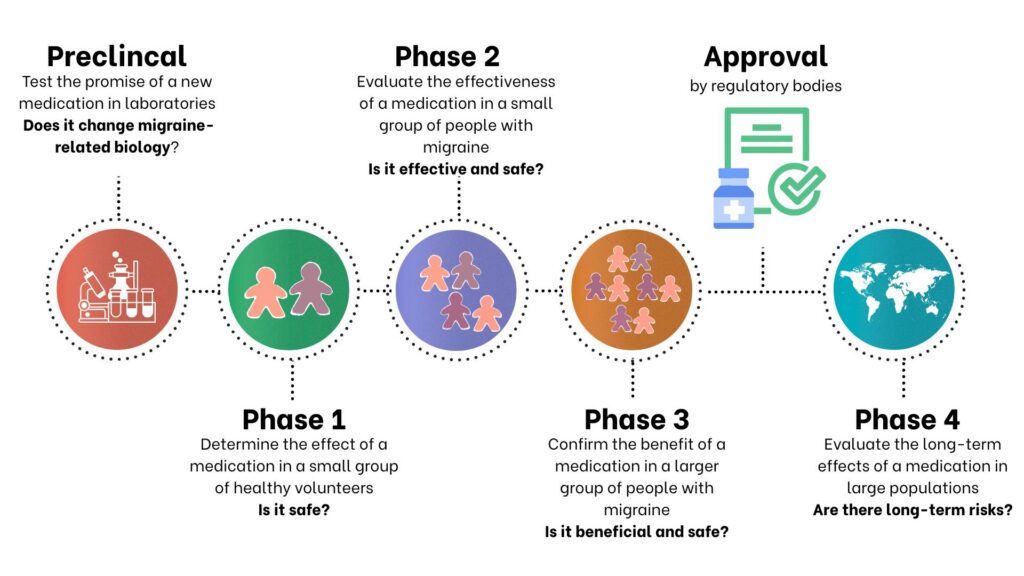
If a medication shows promise in preclinical testing, it will move on to clinical trials. Clinical trials are divided into four phases to ensure safety of participants and effectiveness of a drug. Each phase has its own specific purposes and builds upon the preceding phase.
The key questions answered and goals of each phase of a clinical trial are as follows:
- Phase 1: Is it safe? What dose should be used? Small groups of healthy participants are studied to determine the safety of the drug candidate.
- Phase 2: Does it show signs of working? Is it effective in improving migraine biology in people with migraine? Larger groups of volunteers, including people with migraine, allow researchers to test the effectiveness of the drug at improving migraine-related biology.
- Phase 3: Does it work well and safely compared to existing treatments? Does it provide additional benefits to existing drugs that are already on the market? Large populations are studied to assess if there are improved benefits to most people with migraine.
- Approval by regulatory bodies: Can this drug be put on the market? If there is evidence that a drug candidate meets these criteria in a significant proportion of participants, the medication will be considered for market approval. In the United Kingdom, regulatory bodies like the Medicines and Healthcare products Regulatory Agency (MHRA) oversee the approval of new medications. These regulatory bodies are critical in ensuring treatments are safe and effective for public use. In England and Wales, approval by regulatory bodies is not the final stage. New drugs also need to be assessed and approved by the National Institute for Health and Care Excellence (NICE) to make them available to people being treated by the NHS, often with specific rules.
- Phase 4: What happens after approval in real-world use? Even after approval, drugs continue to be monitored. This is done to look out for rare side effects that may not have been spotted during clinical trials. It also allows real-world data to be collected to refine how medications are used. For example, drugs could be repurposed or better dosing strategies can be discovered to improve their use in migraine management.
Why does this process take so long?
It can take years (and hundreds of millions of pounds) to develop an idea for a new migraine medication into a fully-fledged drug that is prescribed in the clinic. Circling back to the development of the triptans, although they were discovered in the late 1970s, they were only made available to the public in the 1990s. Similarly, CGRP was initially discovered in the early 1980s and convincingly linked to migraine biology in 1990, but the first CGRP-targeting drug (a CGRP monoclonal antibody called erenumab) was only approved for use in 2018. Testing these medications for safety and effectiveness took around 20 to 30 years, highlighting that the process from drug discovery to development can be slow. Many potential drugs fail along the way either in their ability to work well in improving symptoms of a migraine attack, in their safety or in providing more benefits than existing medications. Therefore, time is needed to ensure that beneficial medications are being developed.
What is currently in the discovery pipeline?
There are currently exciting prospects in the migraine treatment pipeline. While much progress has been driven by targeting CGRP, researchers are now exploring new approaches that go beyond pain.
Recent clinical trial data showed the potential for early intervention in migraine care, whereby blocking CGRP signalling during the earliest phase of an attack, prior to the onset of pain demonstrated beneficial effects. Data from the study suggests that the early use of a newer drug class, gepants, may help reduce severity of non-pain symptoms. Additionally, the targeting of a related molecule, Pituitary Adenylate Cyclase–activating Polypeptide (PACAP), has now passed Phase 2 of its clinical trial. This drug is aimed at promoting migraine prevention and has been reported to demonstrate a reduction in the number of monthly migraine days. Alongside this, precision medicine is emerging as a promising approach of improved migraine management by tailoring treatments to individuals based on their specific biology and symptom profiles.
Together, these advances point towards a future where migraine care is more effective and personalised.