Key takeaways:
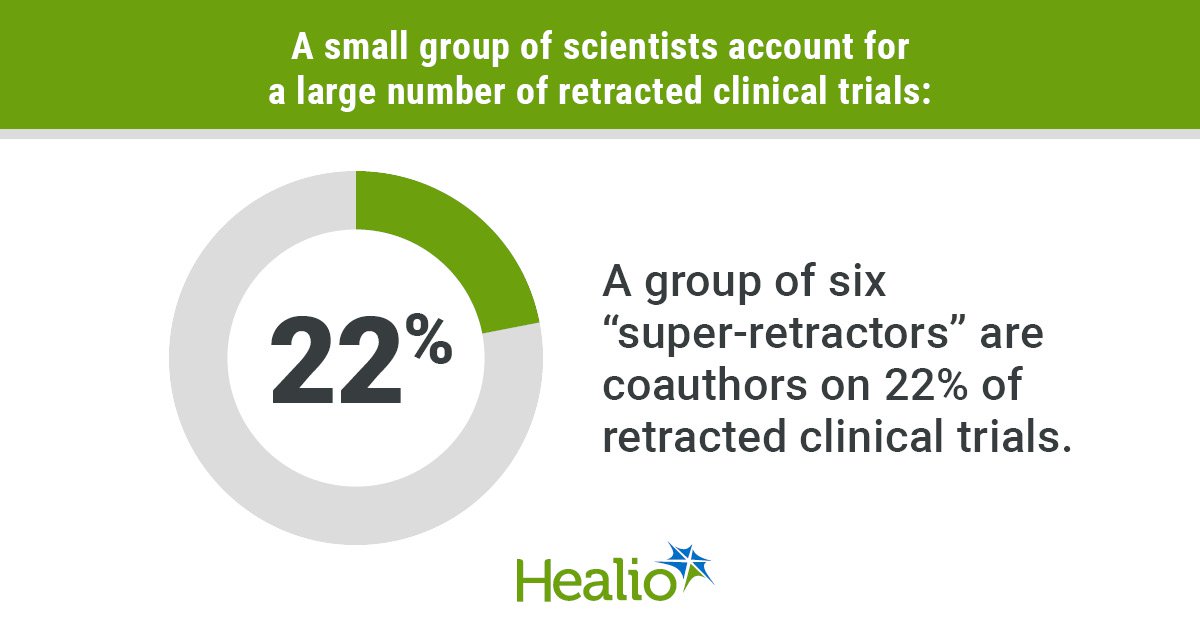
- More than 20% of retracted clinical trials can be linked to a group of six “super-retractors.”
- Fraudulent data can have a widespread impact on guidelines and practice.
A substantial number of retracted randomized clinical trials can be linked to a small group of scientists, results of a retrospective cohort study showed.
Six “super-retractors” have coauthored more than 20% of retracted randomized clinical trials. Additionally, a group of top-cited scientists in their respective fields who have at least 10 retractions have coauthored 25% of retracted randomized clinical trials.

Data derived from Lyu C, et al. JAMA Netw Open. 2026;doi:10.1001/jamanetworkopen.2026.7424.
Altered or fabricated data from these sources have lasted significantly longer in the literature than retracted trials that did not come from these sources.

Ioana Alina Cristea
“The literature is much more unreliable than we realize,” Ioana Alina Cristea, PhD, clinical psychologist and meta-researcher at University of Padova in Italy, told Healio.
Investigating fraud
In 2025, Chang Xu, PhD, executive director at Shanghai Eastern Hepatobiliary Surgery Hospital, and colleagues published findings from VITALITY Study I in The BMJ, which detailed the widespread impact retracted randomized trials could have on future research.
They found retracted trails contaminated 157 guideline documents.
“Retracted trials had a substantial impact on the evidence ecosystem,” Xu and colleagues wrote.
The Committee on Publication Ethics (COPE) has provided guidelines for editors on when retractions should be made, including if there is “clear evidence of major errors, irregularities in the data or images, or any form of misrepresentation [fraud, identity theft, or fictitious authorship] that compromise the reliability of the findings.”
However, trials meeting those guidelines frequently are not retracted, according to study background.
One investigation of 95 randomized controlled trials showed 25% had some concerns and 6% had serious concerns, but only two of those trials had been retracted.
“It’s really difficult to say precisely that this is grounds for retraction or this is grounds for correction,” Cristea said. “Journals themselves are not consistent with each other.”
Retraction Watch keeps an updated “leaderboard” of authors who have the most retractions.
Cristea and colleagues investigated how impactful the most retracted authors are to research using the VITALITY cohort of 1,330 randomized controlled trials.
They used the data to produce three categories of scientists: super-retractors, who have the most retractions on the Retraction Watch leaderboard; scientists in the top 2% or 100,000 of their field based on citations throughout their careers who have at least 10 retractions; and top-cited scientists in their field in 2024 who had at least 10 retractions.
Retractions could not be due to editor or publisher errors.
“We are trying to get at fraudulent and fabricated data,” Cristea said.
Authorship and characteristics of retracted clinical trials served as the primary endpoint.
‘Contamination chain’
Researchers identified 30 super-retractors, 163 top-cited career-long scientists and 174 top-cited authors in 2024.
Super-retractors made up 9% of the career-long cohort and 5% of the recent-year cohort.
Overall, six super-retractors coauthored 22% of retracted randomized trials. Of those trials, 18% included multiple super-retractors.
Those six super-retractors were either in anesthesiology (n = 3) or endocrinology (n = 3).
In the career-long cohort, 18 scientists coauthored 25% of retracted trials. That group of authors also included five super-retractors. A super-retractor was a coauthor on 84% of this group of retracted trials.
The most common fields for those 18 scientists included anesthesiology (n = 4) and cardiovascular system and hematology (n = 4).
In the recent-year cohort, seven scientists coauthored 4% of retracted randomized trials.
Retracted randomized trials that included a super-retractor had a significantly higher likelihood of being published earlier (median, 2000 vs. 2020, P < .001), retracted earlier (median, 2013 vs. 2023; P < .001), having longer time between publication and retraction (median, 5,111 days vs. 482 days; P < .001), and having more citations (median, 21 vs. 5; P < .001).
Likewise, retracted randomized trials that included top-cited career scientists with at least 10 retractions were significantly more likely to be published earlier (median, 2001 vs. 2021, P < .001), retracted earlier (median, 2014 vs. 2023; P < .001), have longer time between publication and retraction (median, 4,748 days vs. 469 days; P < .001), and have more citations (median, 24 vs. 4; P < .001).
“These six super-retractors in our study are very well known, and each of them was researched independently,” Cristea said. “The top-cited scientists with over 10 retractions are perhaps even more worrying, particularly because this is a dynamic list. Maybe next year there will be more of these top-cited scientists who still receive the benefit of being influential researchers, but keep accumulating retractions for reasons that are not errors or mistakes of the journal.”
Researchers acknowledged study limitations, including only analyzing trials that had been retracted.
“We are just looking at what we know,” Cristea said. “Some fields, like anesthesiology and endocrinology, were more scrutinized. Others were not scrutinized at all. Maybe there are a lot of super-retractors or a lot of people whose papers should be retracted because the data are unreliable, and we have no idea.”
Investigations into these fields are critical, she said.
“There may be fields that have not had this alarm call for a number of reasons,” Cristea explained. “Maybe people expect findings to be divergent. Maybe nobody has taken the time to watch.”
Cristea also noted the importance of analyzing the impact top-rated scientists with a lot of retractions have had on the literature.
She encouraged clinicians and researchers to take extra time evaluating studies before implementing them into practice.
“Even findings that look very good and reliable from a clinical point of view should be scrutinized more carefully than ever for the integrity of the data,” Cristea said.
Xu and colleagues wrote an accompanying editorial in JAMA Network Open emphasizing that point.
“Retraction is an effective way to correct the record afterward, significantly reducing citations and curbing the spread of errors,” they said. “Yet, this is insufficient — it requires effort for detection, and more importantly, citation cessation does not mean the infection has vanished. Researchers may have already built on fabricated methods and results or even applied fabricated evidence to clinical practice. To this end, we should not only assess the possibility of fraud but also aim to fully track the research and promptly eliminate the cascade of fraudulent data from the contamination chain.”
For more information:
Ioana Alina Cristea, PhD, can be reached at ioanaalina.cristea@unipd.it.
Ask a clinical question and tap into Healio AI’s knowledge base.
- PubMed, enrolling/recruiting trials, guidelines
- Clinical Guidance, Healio CME, FDA news
- Healio’s exclusive daily news coverage of clinical data