Key takeaways:
- If purchased through direct-to-consumer pharmacies, 80% of generic drugs with cost sharing of at least $15 would have lower out-of-pocket costs.
- Experts discussed the model’s pros and cons.
Direct-to-consumer pharmacies could offer substantial savings for patients taking generic medications, according to experts.
John Lin, MD, MSHP, assistant professor of Health Services Research at The University of Texas MD Anderson Cancer Center, and colleagues recently published a research letter in Annals of Internal Medicine evaluating savings from direct-to-consumer (DTC) pharmacy models.

“As an oncologist, DTC pharmacies have helped many of my patients better afford their cancer drugs. It can be incredibly stressful to have a serious illness, like multiple sclerosis or cancer, and then not be able to afford your medicines,” Lin said. “We wanted to make it easier for patients and prescribers to know when they should turn to DTC pharmacies for help.”
What are DTC pharmacies?
DTC models offer transparent pricing and permit patients to purchase their medications without using their health insurance, in a bid to help patients afford generic prescriptions, Lin and colleagues wrote. However, some have questioned DTC’s usefulness for those who are commercially insured, especially during cost-sharing, when patients must pay only part of the drug’s cost after meeting a deductible.
“Commercial insurance relies on third parties to negotiate benefits packages and prices. You have to pay them to do that. They get involved with both generics and name-brand drugs, and I think over the years, they have shown themselves to be inefficient and expensive, which led to the creation of this DTC … that is run directly by the company, no middleman,” Arthur L. Caplan, PhD, a professor and founding head of the division of medical ethics at NYU Grossman School of Medicine, told Healio.
Caplan said these pharmacies will list the medications they have — almost always generic options — with a base price. Usually, they will add a handling charge as well, “but that’s it.”
“So, roughly speaking, DTC is cheaper and easier to use if you’re taking generics than commercial pharmacy benefit management (PBM) programs,” Caplan said. “If you’re still taking name-brand drugs, I think the PBMs both have more of those available, and they compete fairly well, because the DTC model usually doesn’t try to cover name brands.”
Lin added that “DTC models cut out the middlemen that lower costs for the insurance company but don’t always trickle down to the patient.”
“PBMs made close to $10 billion as middlemen charging for their negotiation between drug manufacturers and pharmacies. I think that is wasteful. It has not brought down health care costs. It hasn’t really given greater access. It hasn’t even really cut back on copays,” Caplan said. “Having a for-profit middleman commercial PBM insurer has just not worked. So, the DTC model just has a lot more going for it.”
However, if patients have not yet met their deductible, paying cash through a DTC pharmacy will not count, Lin said. So, he only recommends using these after a patient has met their prescription deductibles.
“It’s important that doctors get informed about this too, so they can recommend to their patients what is best when they prescribe,” Caplan said. “They may not have time to do that during a doctor-patient encounter, but putting information in the waiting room, putting up some videos that help explain the difference, I think would be very worthwhile.”
Direct comparisons
In the study, Lin and colleagues matched coinsurance or copayment accounts for generic prescription claims from Merative MarketScan encounters and commercial claims in 2024 with 2025 direct purchase prices through the DTC Mark Cuban Cost Plus Drug Company (MCCPDC) based on drug name, quantity, strength and formulation. They analyzed 60,200,969 claims.
The researchers found that purchasing through the DTC pharmacy would have saved patients a median of $6 in about 15% of prescriptions, but savings increased for medications with higher cost sharing. For generic drugs that had cost sharing of at least $15, patients would have seen lower out-of-pocket costs for 80% of the prescriptions if they had been purchased through the DTC pharmacy.
Additionally, when the researchers analyzed generics with cost sharing of at least $100, they found a stark disparity. Through insurance, median out-of-pocket costs were $140. But through the DTC pharmacy, median out-of-pocket costs were $25 — equating to 85% in median relative savings, or $119 in median absolute savings.
“We anticipated there would be savings with direct-to-consumer pharmacies, but what was surprising was the consistency and depth of the savings,” Lin said. “For the highest cost generic drugs, patients who were paying $145 for their copay would only pay $25 through Mark Cuban Cost Plus Drugs.”
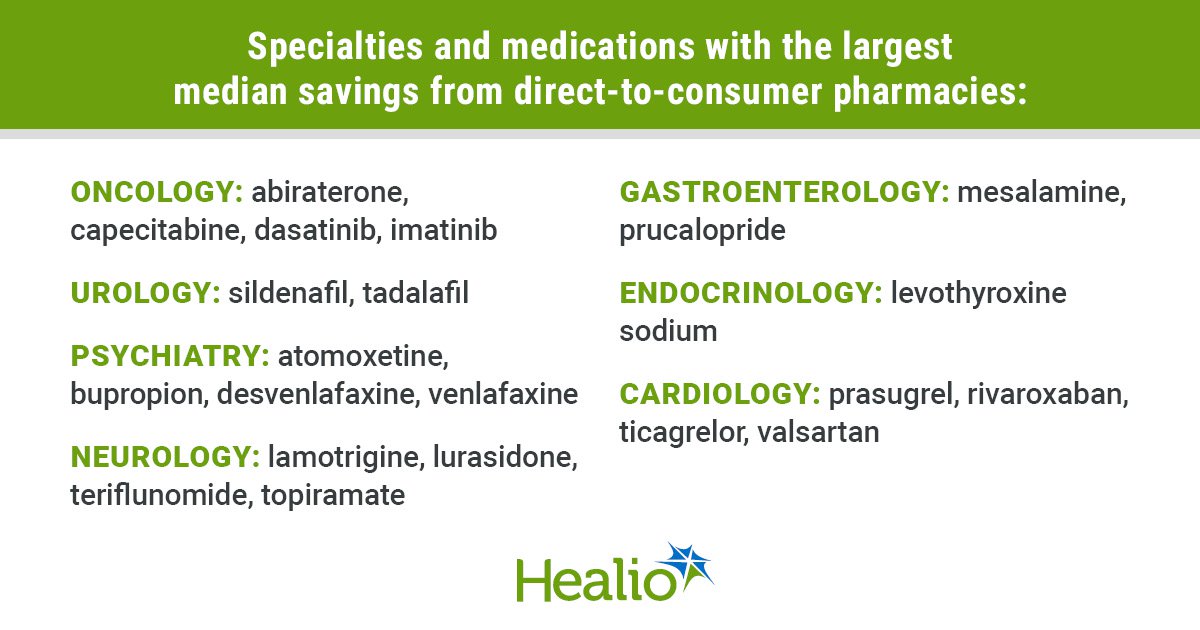
Lin also noted some of the disease areas where patients commonly see large savings for medications purchased through a DTC pharmacy, including the median savings and interquartile range (IQR) for each:
- cardiology ($110; IQR = $87 to $160): prasugrel, rivaroxaban, ticagrelor and valsartan;
- endocrinology ($120; IQR = $114 to $122): levothyroxine sodium;
- gastroenterology ($129; IQR = $84 to $219): mesalamine and prucalopride;
- neurology ($133; IQR = $99 to $279): lamotrigine, lurasidone, teriflunomide and topiramate;
- oncology ($468; IQR = $123 to $1,905): abiraterone, capecitabine, dasatinib and imatinib;
- psychiatry ($136; IQR = $102 to $224): atomoxetine, bupropion, desvenlafaxine and venlafaxine;
- transplant ($100; IQR = $71 to $208): tacrolimus; and
- urology ($139; IQR = $114 to $213): sildenafil and tadalafil.
“Primary care physicians are overburdened and are often unable to speak with all of their patients about prescription costs. We hope that the simplicity of our message can help physicians and patients better understand options available to them,” Lin said. “If [a patient’s] generic coinsurance or copay is higher than $15, they are probably overpaying. If they are paying more than $50, they could potentially get a 70% discount going to a DTC pharmacy.”
Caplan agreed. He said if a patient is paying more than $15 for generic medication, DTC may be a good, cost-saving option.
“If you are reliant on a brand-name drug for which there is no generic, I think you’re probably stuck for now. The best chance at coverage and getting something is the commercial guys,” Caplan said. “What we really need is some AI-driven formula, so that you can always tell which is better for you. Leaving all this up to the consumer to figure out in terms of prices, savings, which drugs are covered by who is impossible.”
For more information:
Arthur L. Caplan, PhD, can be reached at primarycare@healio.com. John Lin, MD, MSHP, can be reached on X at @johnlin08.
Sources/Disclosures
Source:
Healio Interviews
Reference:
Disclosures:
Caplan reports no relevant financial disclosures. Lin reports receiving a topically related grant from the NIH within the past 36 months but outside of the study.
Ask a clinical question and tap into Healio AI’s knowledge base.
- PubMed, enrolling/recruiting trials, guidelines
- Clinical Guidance, Healio CME, FDA news
- Healio’s exclusive daily news coverage of clinical data