Most people spend a lot of time thinking about their hair: the right shampoo, the right cut, the right products. But the scalp? It often gets overlooked entirely. And that’s a problem, because your scalp is where everything begins. Think of your scalp the way you think of soil in a garden. No matter how much attention you give to the plant above ground, if the soil underneath is depleted, compacted, or out of balance, healthy growth simply cannot happen. The same principle applies to your hair. If your scalp is clogged, inflamed, or lacking in circulation, your follicles cannot do their job. At NHLMA, we see this every day in our practice. Patients come in frustrated with thinning, shedding, or slow growth, and what we often find is that the root of the issue (literally) is an unhealthy scalp environment. The good news is that scalp health is something you can actively improve. Here is where to start. Why Scalp Health Is the Foundation of Hair Growth Your hair follicles live inside your scalp. Each follicle is a living structure surrounded by blood vessels that deliver oxygen and nutrients, sebaceous glands that produce natural oils, and a network of cells that regulate the growth cycle. When any part of that environment is compromised, it affects how your hair grows, or whether it grows at all. Common scalp conditions that interfere with hair growth include buildup from products and dead skin cells, excess oil or chronic dryness, scalp inflammation (which can be silent and symptom-free), reduced blood flow to the follicles, and microbial imbalance that disrupts the scalp’s natural ecosystem. Addressing these issues proactively is one of the most effective things you can do to support long-term hair density and health. Source link

12 Ways I Make It as a Sports Mom with Migraine
I often get asked how I make it as a sports mom with migraine. How are you going to all of these games, handling all of these triggers, and surviving in these environments while living with chronic migraine? Just like most things in my life I plan, I try, I fail, and I push myself in order to maintain my quality of life. My children are my happiness and watching them do what they love fills me to my soul! 12 Ways I Make it as a Sports Mom with Migraine Being a sports mom while dealing with migraine attacks can be challenging, but it’s definitely possible to manage both responsibilities with some careful planning and self-care. Here are some tips on how I navigate this situation. Prioritize Self-Care Get Enough Sleep: Ensure you’re getting regular, good-quality sleep. Lack of sleep can be a trigger for migraine. Prioritize good-quality sleep. Establish a bedtime routine and create a comfortable sleep environment. Stay Hydrated: Dehydration can also trigger migraine, so make sure you’re drinking enough water throughout the day. Ensure you’re drinking enough water and eating balanced meals. Dehydration and skipped meals can also trigger migraine attacks. Manage Stress: Practice relaxation techniques like deep breathing, meditation, or yoga to help reduce stress levels. Regular Exercise: Engage in regular low-intensity exercises like walking, swimming, or yoga. These can help manage stress and potentially reduce the frequency of migraine attacks. Nutrition Eat regular, balanced meals. Skipping meals can trigger migraine. I typically try to follow the Dizzy Cook, HYH diet. Identify and avoid migraine-trigger foods. Common culprits include MSG, caffeine, alcohol, aged cheese, processed meats, and artificial sweeteners. My functional medicine doctor helped me with this. Communicate with Coaches and Team Let your child’s coaches and teammates know about your condition. They can offer support and understanding if you need to take a step back occasionally. Organize schedules and plan in advance. This includes knowing the practice and game times, transportation arrangements, and any other logistical details. Plan Ahead Organize schedules and plan in advance. This includes meal planning, transportation, and coordinating with other parents if necessary. Sports Mom Migraine Toolkit Carry essentials like pain relievers, water, snacks, and any prescribed medications for migraine. Protect Yourself from Bright Lights Wear sunglasses or a visor during outdoor games to reduce exposure to bright sunlight, which can be a migraine trigger. Protect yourself from Sound Noise-canceling headphones, earbuds Protect yourself from Smells Indoor smells Outdoor smoke and smells Dress in layers Bring an Umbrella and fan Listen to Your Body Recognize early signs of a migraine prodrome and take steps to address it promptly. Don’t push yourself too hard if you’re feeling unwell. Designate a Support System Don’t be afraid to ask for help. Whether it’s from your partner, family, or other parents, having a support system in place is crucial. For each sport and team my kids play on, I seek support. Identify someone who can step in if you’re unable to attend a game or practice due to an attack. This could be a spouse, family member, or another parent. Explore Treatment Options Consult a healthcare provider about treatment options. This might include medications, lifestyle changes, or alternative therapies. Set Realistic Expectations It’s okay to miss a game or practice if you’re not feeling well. Communicate openly with your child and their team about your condition. Practice Mindfulness Create a Relaxation Routine: Practice relaxation techniques like deep breathing, meditation, or visualization to help reduce stress levels. Practice Mindfulness: Mindfulness techniques can help you stay present and reduce anxiety about potential migraine attacks. Stay present in the moment. Sports Moms Take Breaks Allow yourself breaks during games or practices to rest and recharge. Find a quiet place if possible. Maintain Open Communication Talk to your child about your condition. They may have questions or concerns, and being open can help strengthen your relationship. Remember, it’s important to consult with a healthcare provider for personalized advice and treatment options. They can help you manage your migraine effectively while still being there for your child’s sports activities. Sports Mom by Sport With every season, comes new challenges. Each season I limit sports exposure to triggers by identifying them and being prepared. Here’s the type of mom I currently am… Be sure to follow on Instagram for more photos and updates. Volleyball Mom with Migraine Baseball Mom with Migraine Softball Mom with Migraine Football Mom with Migraine Swim Mom with Migraine Indoor Swim Mom Floor Hockey Mom with Migraine Overall, being a sports mom is my favorite job. It takes work but there is not better place for me than watching my kids live their best lives. Source link
Should gastroenterologists prescribe GLP-1s to their patients?
Column Editorials Add topic to email alerts Receive an email when new articles are posted on Please provide your email address to receive an email when new articles are posted on . “ data-action=”subscribe”> Subscribe We were unable to process your request. Please try again later. If you continue to have this issue please contact customerservice@slackinc.com. Back to Healio More from Column Editorials View all This month’s Healio Exclusive in Healio Gastroenterology poses a highly topical question. GLP-1 receptor agonists have revolutionized the treatment of obesity and related conditions, including type 2 diabetes, major adverse cardiovascular events, obstructive sleep apnea, metabolic dysfunction-associated steatotic liver disease, osteoarthritis and polycystic ovarian syndrome. The benefits of this drug class seem to far outweigh adverse events, which are often gastrointestinal. For some patients, including those with MASLD, gastroesophageal reflux disease or inflammatory bowel disease, there is evidence that these drugs may provide benefit. I personally have witnessed significant improvement in gastrointestinal symptoms for some of my patients with Crohn’s disease, ulcerative colitis and ileoanal pouch dysfunction. Furthermore, given the association between BMI and risk for gastrointestinal cancers, use of GLP-1s may prevent these malignancies. This raises the question: Should gastroenterologists prescribe these drugs as well? GLP-1s often seem to be under the purview of endocrinologists, weight management specialists or primary care providers. In one camp, we hear from gastroenterologists who subspecialize in obesity and feel we should fully embrace this drug class and be comfortable prescribing them. However, we also hear concerns about how GLP-1s are being marketed directly to patients through online health platforms, leading to little or no oversight of the prescription. One could argue this is a sign of primary care provider shortage and another reason for gastroenterologists to take ownership of prescribing GLP-1s. Given the broad number of indications for these drugs, it may be best for the primary care provider to “be the quarterback” and handle the prescribing. Certainly, gastroenterologists should embrace drugs such as tirzepatide and semaglutide in the sense that they should encourage patients with overweight or obesity to try them when the question is raised. As mentioned by Michael Camilleri, MD, DSc, in the cover story, use of GLP-1s fits nicely within the spectrum of treatments that should be offered to these patients after diet and lifestyle modifications but before endoscopic or surgical bariatric procedures. We also should be familiar with and comfortable discussing potential side effects of these medications, which include nausea, vomiting, diarrhea, constipation, indigestion, abdominal pain, fatigue and belching. We can talk patients through some of these side effects and reassure them that generally, they ease with time. We also should be aware of less common and more severe side effects such as biliary problems, pancreatitis and allergic reactions. Ultimately, the decision for a gastroenterologist to prescribe GLP-1s is a personal one and will depend on their patients and the availability of primary care providers who are comfortable with this class of drugs. Further research into the effect of the use of this drug class on gastrointestinal cancer prevention is warranted, too. For more information: Edward V. Loftus Jr., MD, is the Maxine and Jack Zarrow Family Professor of Gastroenterology at the Mayo Clinic and chief medical editor of Healio Gastroenterology. He can be reached at loftus.edward@mayo.edu. More from Column Editorials View all Published by: Sources/Disclosures Source: Expert submission Disclosures: Loftus reports consulting for AbbVie, Alvotech, Amgen, Boehringer Ingelheim, Bristol Myers Squibb, Celltrion Healthcare, Eli Lilly & Co., Fresenius Kabi, Gilead Sciences, Janssen and Takeda Pharmaceuticals; and receiving research support from AbbVie, Bristol Myers Squibb, Celgene/Receptos, Gilead, Janssen and Takeda. Ask a clinical question and tap into Healio AI’s knowledge base. PubMed, enrolling/recruiting trials, guidelines Clinical Guidance, Healio CME, FDA news Healio’s exclusive daily news coverage of clinical data Learn more Add topic to email alerts Receive an email when new articles are posted on Please provide your email address to receive an email when new articles are posted on . “ data-action=”subscribe”> Subscribe We were unable to process your request. Please try again later. If you continue to have this issue please contact customerservice@slackinc.com. Back to Healio Source link

What Is Neuromodulation? A Guide to Advanced Pain Relief
Chronic pain affects millions of Americans, impacting every aspect of daily life—from sleep and work to relationships and mental health. When medications, physical therapy, and injections don’t provide adequate relief, many patients feel they’ve run out of options. Neuromodulation is a groundbreaking approach to pain management that offers hope when traditional treatments fall short. At Pain Specialists of America, we understand the devastating impact of persistent pain on our Central Texas patients. As pioneers in interventional pain management, we offer advanced neuromodulation therapies that can transform your relationship with pain and help you reclaim your life. Here’s what we’ll address in this blog post: Neuromodulation uses electrical stimulation to interrupt pain signals before they reach your brain Common types include spinal cord stimulation (SCS) and dorsal root ganglion (DRG) stimulation These treatments can reduce pain by 50-70% for conditions like failed back surgery syndrome and complex regional pain syndrome Pain Specialists of America was first in Texas to integrate Abbott’s advanced Proclaim™ Plus SCS system Patients often experience improved function, reduced medication use, and better quality of life Minimally invasive outpatient procedure with a trial period to test effectiveness before permanent implantation Not everyone is a candidate—consultation with a pain specialist determines eligibility What Is Neuromodulation? Neuromodulation is a minimally invasive medical therapy that uses specialized devices to deliver gentle electrical pulses to specific nerves or areas of the spinal cord. These pulses modify or “modulate” pain signals, preventing them from reaching your brain or changing how your brain interprets them. Think of neuromodulation like a traffic controller for your pain signals. When you experience pain, nerve fibers send messages through your spinal cord to your brain. Neuromodulation devices intercept and modify these signals, reducing your perception of pain without the side effects of medications. Modern neuromodulation systems offer: Personalized programming to target your specific pain Wireless control through discreet remote controls or smartphone apps Rechargeable or long-lasting battery options MRI-compatible options for future diagnostic needs How Does Neuromodulation Work for Pain Relief? Neuromodulation works through precisely targeted electrical stimulation that interrupts the pain signaling pathway. Here’s how the process typically works: Evaluation: Our pain specialists thoroughly assess your condition, medical history, and previous treatments to determine if you’re a candidate. Trial period: Before permanent implantation, you’ll undergo a temporary trial (usually 5-7 days) with external leads placed near your spinal cord or specific nerves. Assessment: If you experience significant pain relief during the trial (typically 50% or greater reduction), you may proceed to permanent implantation. Implantation: In an outpatient procedure, a small device (similar in size to a pacemaker) is placed under your skin, usually in the lower back or buttock area. Thin wires (leads) connect to specific nerve targets. Programming: Your device is programmed to deliver customized stimulation patterns based on your unique pain patterns and response. The stimulation itself may feel like a gentle tingling, buzzing sensation, or—with newer systems—may not be felt at all while still providing pain relief. Most importantly, you remain in control, with the ability to adjust settings or turn the system on and off as needed. Benefits of Neuromodulation for Chronic Pain: Patients who respond well to neuromodulation often experience transformative results: Significant pain reduction – Studies show 50-70% pain relief for many patients Reduced dependence on pain medications – Many patients decrease or eliminate opioid use Improved physical function – Return to activities that pain previously limited Better sleep quality – Less pain disruption during nighttime hours Enhanced mood – Decreased depression and anxiety associated with chronic pain Increased independence – Less reliance on caregivers for daily activities Long-term solution – Provides sustainable relief without building tolerance Reversible and adjustable – Can be modified or removed if needed Most importantly, neuromodulation offers hope for those who believed they would never find relief. As a minimally invasive option, it bridges the gap between medications and major surgery. Neuromodulation vs Other Treatment Options: Treatment Approach How It Works Duration of Relief Invasiveness Side Effects Neuromodulation Interrupts pain signals Long-term, sustainable Minimally invasive Minimal; typically mild discomfort at implant site Opioid Medications Block pain receptors Short-term; tolerance develops Non-invasive Constipation, sedation, dependence, addiction risk Steroid Injections Reduce inflammation Temporary (weeks to months) Minimally invasive Minimal; blood sugar elevation, limited number of treatments Surgical Intervention Corrects structural issues Potentially permanent if successful Highly invasive Significant recovery time, risk of failed back surgery syndrome Physical Therapy Improves function, strength Variable; requires ongoing work Non-invasive Limited effect on severe nerve pain Types of Neuromodulation Devices and Techniques Several neuromodulation approaches are available, each designed to address specific pain conditions: Spinal Cord Stimulation (SCS): The most common form of neuromodulation, SCS delivers mild electrical pulses to the spinal cord. This is particularly effective for: Dorsal Root Ganglion (DRG) Stimulation: This targets the dorsal root ganglion, a cluster of nerve cells near where nerves enter the spinal cord. DRG stimulation excels at treating: Complex regional pain syndrome Groin or pelvic pain Post-surgical pain Foot and ankle pain Peripheral Nerve Stimulation: This targets specific peripheral nerves outside the spinal cord, beneficial for: At Pain Specialists of America, we offer comprehensive evaluation to determine which neuromodulation approach is most appropriate for your specific pain condition and anatomy. Who Is a Good Candidate for Neuromodulation? Not everyone with chronic pain will benefit from neuromodulation. Ideal candidates typically: Have tried and failed conservative treatments (medications, physical therapy, injections) Have a clearly defined pain source that can be targeted Have no untreated drug dependency issues Have realistic expectations about pain reduction Have no psychological conditions that would interfere with treatment Have passed a successful trial stimulation period During your consultation at Pain Specialists of America, our experts will conduct a thorough evaluation to determine if neuromodulation is right for you. This includes reviewing your medical history, previous treatments, diagnostic tests, and performing a physical examination. Taking the Next Step Toward Pain Relief Living with chronic pain isn’t something you should have to accept as your “new normal.” Neuromodulation represents a significant

Facts About a New Osteoporosis Treatment
May is Osteoporosis Awareness and Prevention Month. Ben Swanson is a dentist by trade, but bone health has his heart. As the CEO and co-founder of the drug development company Skeletalis, Swanson and his team are developing a bone-targeted technology that will protect and rebuild bone in people with musculoskeletal diseases like osteoporosis. “The core logic behind what we’re doing is taking musculoskeletal skeletal health broadly into the era of precision medicine that we’ve seen across a number of other diseases,” Swanson said. “With a biology-focused approach to understanding how the disease happens, we’re designing a platform that enables us to get drugs there in a very targeted way, and the end result is we create drugs and therapies that enable freedom from fractures.” And this is really important because most people don’t even know they have the bone disease until a fracture or break happens. And about 1 in 3 women over 50 will fracture a bone because of osteoporosis. “Bone disease hides in plain sight. It doesn’t often hurt, but it is a disease — and fractures are something that affects everyone. Everybody has a family member or someone they’re close to who has suffered from a fracture, and the consequences are tremendous,” Swanson said. “It could be a life-ending event, and we don’t really have therapies that have kept up with the rest of science.” We talked with Swanson about the need for advancements in treatment options for osteoporosis, the pros of precision therapy and how biotechnology is changing the way we treat bone disease. This interview has been edited for clarity and length. HealthyWomen: As co-founder of Skeletalis, what was your inspiration to start a company that focuses on treating musculoskeletal diseases? Ben Swanson: I think my inspiration was really the fascination with the idea that bone is an organ that is constantly remodeling — it’s constantly changing and adapting. And as someone who was studying bone treatments, it became clear there was a tremendous opportunity to make a drug that’s more specific and precise to musculoskeletal diseases like osteoporosis, given that it impacts so many people. The idea is that, if you can get a drug to the place where the disease happens on the skeleton, on the physical surface of the skeleton, you may be able to improve both the efficacy and the ability to treat disease and reduce unwanted side effects. HW: Advancements in treatment options for osteoporosis haven’t seen the same level of innovation as other areas of medicine. Why has progress been slower regarding treatments for osteoporosis and bone health? Swanson: Osteoporosis is not a disease where we can see a change in a simple blood test, like lowering cholesterol. We can’t measure a tumor changing shape or survival necessarily. We’re trying to prove strength and reduce fractures, but fractures are not happening every day, and in fact, fractures are the failure of treatment, and we don’t study a lot of other drugs in terms of their failure. Research has been historically slow in this field because of the requirement to have long clinical trials, and one of the things that we are very excited about in osteoporosis is a recent change in the regulatory framework called the SABRE initiative, which has made trials much faster and cheaper and really opens the doors to modern development. The other thing that’s really important here is that, historically, osteoporosis therapies work by shutting down the bone. With recent advances in our understanding of why bone degenerative diseases happen and how we go from normal maintenance mode into some degenerative or imbalance mode, we can design much more precise therapies. For the first time, we have that combination of exciting new science and new understanding of why these diseases happen and the regulatory environment that enables us as a small company to make a meaningful difference. HW: Tell us how the company’s Osteoclast-Activated Skeletal Intervention System (OASIS) approach is different from traditional osteoporosis treatments. Swanson: If we think about traditional drugs — and that could be any drug — they often affect the whole body, so it requires more of the drug and there’s exposure to other sites. The way we think about treatment with our OASIS technology is to localize therapy in a precise and thoughtful way in the skeleton and to the places where osteoclasts — the cells that are responsible for osteoporosis — are actually forming. We think about this not just as an osteoporosis medication but really as a platform technology for precision skeletal medicines across diseases. We see a tremendous opportunity across a woman’s lifespan as different skeletal diseases manifest and all of those require safety in a precise or targeted approach. HW: What role does screening play in the prevention of bone loss before fractures occur? Swanson: Fractures are the failure of the skeleton, and for many people fractures are the beginning of the end. Some people will die within the first year of their fracture, and an overwhelming number of patients will never return home. It’s a tremendous cost burden — we’re taking people out of their communities, out of their families, out of their jobs. The biggest opportunity that we see is to prevent that first fracture from ever happening. We have the opportunity as a clinical community to shift osteoporosis care from reactive treatment to prevention and thinking about how we stop or reverse the disease before entering that fracture cascade because after the first fracture the likelihood of the second is even higher. We also have to make screening available to women earlier and more often. If we’re only looking at late stages to someone who’s 10 to 15 years beyond menopause, we can only intervene at that time, so we have to be thinking about earlier screening and earlier detection awareness to empower patients to be asking for these things. That really is what will enable prevention, but it also becomes a normal part of perimenopause or even premenopause. HW: Some women

Tricks for a Better Halloween with Migraine Dos and Don’ts
Tricks for a Better Halloween with Migraine Dos and Don’ts Halloween can be a fun and exciting holiday for many people, but for individuals who suffer from migraines, it can present some unique challenges. Migraines are neurological disorders characterized by severe headaches, often accompanied by other symptoms like nausea, sensitivity to light, and sound. Tricks for a Better Halloween with Migraine Dos and Don’ts Remember, everyone’s migraine triggers and symptoms are unique, so it’s important to pay attention to your own body and adjust your Halloween plans accordingly. With some careful planning and consideration, you can still enjoy the holiday while minimizing the risk of triggering a migraine. Source link

CRC screening rates negatively impacted by racial disparities
Add topic to email alerts Receive an email when new articles are posted on Please provide your email address to receive an email when new articles are posted on . “ data-action=”subscribe”> Subscribe We were unable to process your request. Please try again later. If you continue to have this issue please contact customerservice@slackinc.com. Back to Healio Key takeaways: Non-white individuals are less likely to undergo CRC screening and colonoscopy than white individuals. However, non-white individuals are more likely to use noninvasive testing modalities. CHICAGO — Even as colorectal cancer screening rates have risen among older adults across race and ethnicity, racial disparities in cancer screenings have not improved comparatively, according to data presented at Digestive Disease Week. An analysis of 2015-2023 National Health Interview Surveys showed that despite an annual 1.6% increase in CRC screening overall, individuals who identify as Black, Hispanic or Asian are still less likely to undergo screening than white individuals. Even as colorectal cancer screening rates have risen among older adults across race and ethnicity, racial disparities in cancer screenings have not improved comparatively. Image: Robert Stott. “We found colorectal cancer screening rate growth in all racial groups with an increased use of colonoscopy and noninvasive screening modalities,” Sophie Montgomery, MD, internal medicine resident at Beth Israel Deaconess Medical Center, said during a presentation. “We did not detect narrowing of racial disparities in colorectal cancer screening overall or for any specific modality. I think what this analysis highlights is that noninvasive modality alone has not addressed barriers in colorectal cancer screening. “The existence of these tests isn’t going to solve our problems,” she added. “What we need is robust implementation programs.” Montgomery and colleagues analyzed CRC screening trends by self-reported race among adults aged 50 to 75 years. The analysis included 45,398 participants who completed surveys in 2015, 2018, 2021 and 2023. The overall rate of CRC screening improved during the survey period — rising from 60.8% in 2015 to 72.2% in 2023 — reflecting a 1.6% (95% CI, 1.3%-1.8%) annual increase. Increases were observed across all racial groups, including non-Hispanic white (64% to 75%), non-Hispanic Black (59.7% to 71.7%), Hispanic/Latino (45.4% to 61.2%) and non-Hispanic Asian (53% to 66.1%), with no significant differences detected by race. However, compared with white individuals, CRC screening prevalence was 4.1% lower among Black individuals, 11.5% lower among Asian individuals and 15% lower among Hispanic individuals. Researchers also did not detect significant differences in noninvasive screening trends by race, which rose across all groups. However, rates of noninvasive screening were higher among all racial groups compared with white individuals (Hispanic, 4.6% higher; Asian, 3% higher; Black, 1.8% higher), although colonoscopy rates remained lower (Hispanic, 20% lower; Asian, 14.9% lower; Black, 6.9% lower). Overall, results show that systemic changes are necessary for CRC screening to be equally accessed by all. “If we want to address racial disparities, we need to address the social determinants of health more broadly,” Montgomery said. Published by: Sources/Disclosures Source: Montgomery S, et al. Rising use of stool-based testing is not bridging racial disparities in colorectal cancer screening: The National Health Interview Survey 2015-2023. Presented at: Digestive Disease Week; May 2-5, 2026; Chicago. Disclosures: Healio could not confirm relevant financial disclosures at time of publication. Ask a clinical question and tap into Healio AI’s knowledge base. PubMed, enrolling/recruiting trials, guidelines Clinical Guidance, Healio CME, FDA news Healio’s exclusive daily news coverage of clinical data Learn more Add topic to email alerts Receive an email when new articles are posted on Please provide your email address to receive an email when new articles are posted on . “ data-action=”subscribe”> Subscribe We were unable to process your request. Please try again later. If you continue to have this issue please contact customerservice@slackinc.com. Back to Healio Source link

Muscle Pain vs Nerve Pain: How to Tell the Difference
Are you struggling to understand whether your discomfort is muscle pain or nerve pain? Knowing the difference is crucial for finding effective relief and preventing long-term complications. Before we get into specifics, here’s a quick look at these two types of pain: Muscle pain typically feels dull and achy, while nerve pain feels sharp, burning, or electric Muscle pain is usually localized, but nerve pain often radiates along nerve pathways Muscle pain generally improves with rest within days; nerve pain tends to persist or worsen Numbness, tingling, and weakness typically accompany nerve pain but not muscle pain What is Muscle Pain? Muscle pain (myalgia) is discomfort that originates in your muscles or related soft tissues. It typically results from physical strain, overuse, tension, or injury to the muscle fibers. Common causes of muscle pain include: Overexertion during physical activity Sports injuries or accidents Poor posture or repetitive movements Stress and tension Inflammatory conditions like fibromyalgia or myositis Infections like the flu The hallmark of muscle pain is its typically dull, aching nature. When you press on the affected area, you’ll often feel tenderness or soreness. Muscle pain usually responds to rest and basic home care in a matter of days, unless there’s a more serious underlying issue such as a significant tear or chronic condition. What is Nerve Pain? Nerve pain (neuropathic pain) occurs when there’s damage or compression to your nerves. Unlike muscle pain, nerve pain stems from problems with the nervous system itself rather than surrounding tissues. Common causes of nerve pain include: Pinched nerves from herniated discs or bone spurs Diabetic neuropathy Shingles (post-herpetic neuralgia) Carpal tunnel syndrome Multiple sclerosis Chemotherapy side effects Infections affecting nerves Traumatic injuries that damage nerves Nerve pain has a distinctive quality that patients often describe as sharp, shooting, burning, or electric shock-like sensations. It may include other unusual sensations like tingling, numbness, or “pins and needles.” Unlike muscle pain, nerve pain often radiates along the pathway of the affected nerve—such as down an arm or leg—and tends to be persistent or recurrent rather than temporary. How to Tell the Difference Between Muscle and Nerve Pain? Distinguishing between muscle pain and nerve pain can help you communicate more effectively with healthcare providers and get on the right treatment path sooner. Here are the key differences to watch for: Sensation and Quality: Muscle pain: Typically feels dull, achy, crampy, or sore Nerve pain: Usually sharp, shooting, burning, stabbing, or electric-like Location and Radiation: Muscle pain: Generally localized to the affected muscle group (e.g., sore neck muscles) Nerve pain: Often radiates along nerve pathways (e.g., pain shooting from neck down the arm) Associated Symptoms: Muscle pain: May include stiffness, spasms, tenderness, and reduced range of motion Nerve pain: Often accompanied by tingling, numbness, prickling sensations, or weakness Response to Rest and Movement: Muscle pain: Typically improves with rest and gentle stretching Nerve pain: May not improve with rest and sometimes worsens with certain movements Duration and Pattern: Muscle pain: Usually improves within days with appropriate self-care Nerve pain: Tends to persist, may become chronic, and often doesn’t resolve without treatment A simple self-test: If your pain responds positively to rest and feels better after a few days, it’s more likely muscle-related. If it persists regardless of rest and includes unusual sensations like tingling or numbness, nerve involvement is more likely. Benefits of Proper Pain Diagnosis and Treatment: Understanding whether you’re dealing with muscle pain or nerve pain offers several important advantages: Targeted Relief: The right diagnosis leads to the right treatment approach, providing faster and more effective relief Prevention of Chronic Issues: Early and appropriate intervention reduces the risk of acute pain becoming chronic Minimized Medication Dependence: Precise treatments mean less reliance on pain medications, especially opioids Improved Function: Proper treatment addresses the root cause, helping restore normal daily activities and mobility Better Quality of Life: Effective pain management allows you to sleep better, move more freely, and enjoy life again At Pain Specialists of America, our physician team specializes in accurate diagnosis using advanced techniques, including specialized imaging and diagnostic nerve blocks when necessary. This precision allows us to create personalized treatment plans that target the specific source of your pain. Muscle Pain vs Nerve Pain Treatment Options: Treatment approaches differ significantly between muscle and nerve pain. Here’s how we approach each type: For Muscle Pain: Conservative Approaches: Rest, ice/heat therapy, gentle stretching, and over-the-counter anti-inflammatory medications Physical Therapy: Targeted exercises to strengthen and rehabilitate affected muscles Trigger Point Injections: Direct injection of medication into painful muscle knots Joint Injections: Relief for muscle pain related to joint dysfunction Regenerative Treatments: Platelet-Rich Plasma (PRP) injections to promote natural healing of damaged muscles Soft Tissue Injections: Targeted relief for chronic muscle pain in the limbs and trunk For Nerve Pain: Nerve Blocks: Targeted injections to interrupt pain signals from specific nerves Epidural Steroid Injections: Reduce inflammation around compressed spinal nerves Radiofrequency Ablation: Precision technique that uses heat to interrupt pain signals Spinal Cord Stimulation: Implantable device that masks pain signals before they reach the brain Peripheral Nerve Stimulation: Similar to spinal stimulation but targets specific peripheral nerves Dorsal Root Ganglion Blocks: Specialized treatment for nerve root pain Lidocaine Infusion: For management of severe nerve pain Our interventional approach means we identify and treat the root cause of your pain rather than just masking symptoms. For patients in Central Texas, this means access to advanced treatments without the need for surgery or heavy reliance on medications. Who is a Good Candidate for Interventional Pain Management? You may benefit from interventional pain management at Pain Specialists of America if: Your pain has lasted more than three days and is not improving with rest and over-the-counter medication You’re experiencing numbness, tingling, or weakness along with your pain Your pain radiates from one area to another (like from your back down your leg) You’ve tried conservative treatments without adequate relief You want to avoid surgery if possible You’re looking to reduce reliance on pain medications Your quality of

The Type 2 Inflammation Connection
May 18–22, 2026, is Type 2 Inflammation Awareness Week. When your body is facing illness, injury or invasion from anything that doesn’t belong, like viruses, bacteria or parasites, inflammation is the body’s way of fighting back to start the healing process. The immune system responds to illness and injury by sending inflammatory cells to stop the threat. The result is called acute inflammation, which you might experience as: Pain or tenderness Fever Swelling Reddened skin at the injury site While uncomfortable, this type of inflammation is a healthy response. It disappears once the body heals. But with chronic inflammation, your body keeps sending inflammatory cells for months or years even in the absence of a threat. In this case, the process that is designed to heal your body can damage it. Healthcare providers (HCPs) call this type 2 inflammation. “I describe type 2 inflammation as a specific kind of swelling in the body, often associated with allergic conditions, that can occur in multiple organs at once, such as the skin, nose, airways, and lungs,” said Payel Gupta, M.D., triple-board-certified allergist and assistant clinical professor at SUNY Downstate Medical Center and Mt. Sinai Medical Center in New York. “If you have this type of inflammation in one part of your body, you may also have it in another part of your body.” Connected conditions With your skin, nose, airways and lungs as possible sites for type 2 inflammation, the list of type 2 inflammation-related conditions — including those that often occur together — is substantial. Common coexisting conditions include: Allergies – An allergy is a reaction of the immune system to a normally harmless substance, like certain foods or plants. People who don’t have that allergy generally won’t react to the substance. Asthma – Asthma is a lung condition that causes inflammation and narrowing of the lung’s airways, leading to breathing challenges that can be mild or severe. Chronic rhinosinusitis with nasal polyps (CRSwNP) – In this chronic inflammatory condition, benign growths called nasal polyps form in your sinuses or nose and can cause disruptive symptoms, like sinus pressure and difficulty breathing. Even after surgery to remove them, nasal polyps often grow back. Chronic obstructive pulmonary disease (COPD) – In this disease, airways and other parts of your lungs become damaged so that breathing becomes difficult. Smoking is the most common cause of COPD but there are also other causes, like environmental pollutants. Eczema – Eczema is a chronic inflammatory disease that causes dry, itchy inflamed skin. Atopic dermatitis is the most common form of eczema. Eosinophilic esophagitis (EoE) – This chronic condition happens as a response to triggers such as certain foods or environmental allergens. A person’s esophagus is flooded with white blood cells, causing painful swelling of the esophagus. It can become difficult to eat or swallow comfortably. Prurigo nodularis – This condition, which causes raised, itchy skin bumps, can occur anywhere on your body but is most common on the abdomen, arms and legs. Urticaria – Urticaria is the medical term for hives, which are red, itchy welts that can appear anywhere on your body, often occurring then disappearing. Over a period of weeks or even months, hives can reappear again and again, often without an obvious cause. When this happens, it’s called chronic spontaneous urticaria. According to Gupta, when people have two or more of these conditions, HCPs should consider whether underlying type 2 inflammation could be making these conditions worse. “Environmental triggers such as allergens like pollen, pet dander, dust mites or mold, as well as pollution or infections, can trigger or worsen type 2 inflammation,” she said. “In these cases, it’s important to calm the underlying type 2 inflammation as much as possible to lessen the severity of the coexisting conditions.” Lack of awareness of type 2 inflammation among both patients and HCPs can contribute to delayed diagnosis, especially if you have more than one condition. This lack of awareness also means the conditions can take a big toll on your quality of life and you may not understand that getting specialized care could potentially make your chronic inflammatory conditions much more manageable. Diagnosing type 2 inflammation Treating underlying inflammation requires an HCP to identify inflammation that extends beyond just one condition, like asthma or EoE. One way that HCPs figure out if you have widespread inflammation is to measure the number of eosinophils in your blood. Eosinophils are a type of white blood cell that defend your body from allergens. They can also be a marker for type 2 inflammation. When your blood contains too many eosinophils, that will help your HCP make the diagnosis of type 2 inflammation. Another way your HCP might be able to identify type 2 inflammation in your body is by using a breathing test called a fractional exhaled nitric oxide test. This test measures the amount of nitric oxide you exhale with each breath. The more nitric oxide, the more swollen your airways are, Gupta said. Which type of HCP can diagnose or manage type 2 inflammation-related conditions? According to Gupta, you don’t always need to see a specialist right away if your conditions are well-controlled.“But if you ever feel your conditions are not controlled or responding to your current treatments, you should ask for a referral to a specialist.” You may already be seeing a specialist, of course. For example, people with eczema might see a dermatologist, someone with EoE probably sees a gastroenterologist and someone with COPD probably sees a pulmonologist. Having a multidisciplinary medical team behind you is important when dealing with complicated conditions like type 2 inflammation, so you might want to see an allergist, too. Allergists can help manage all type 2 inflammation-related conditions and should have updated knowledge of medications that can help. Gupta said, “Many of the medications used in type 2 inflammation can help with more than one condition, but they’re often biologics that require specialized knowledge and access.” Disease control, not cure Unfortunately, there is no cure for

Best Hair Loss Treatments For Men
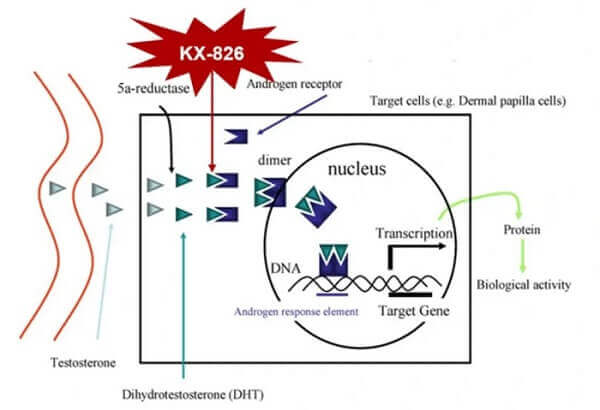
Hair loss is incredibly common in men, yet many delay treatment until thinning becomes more advanced. The good news is that modern, non-surgical hair loss treatments can slow progression, improve scalp health, and support stronger hair growth, especially when started early. At NHLMA, we take a medical, individualized approach to male hair loss. Below, we break down what causes hair loss in men, how to recognize the stages, and the most effective non-surgical options available today. Understanding Male Pattern Hair Loss The most common form of hair loss in men is androgenetic alopecia, often referred to as male pattern hair loss. It is driven by a combination of genetics and sensitivity to DHT (dihydrotestosterone), a hormone that gradually shrinks hair follicles over time. As follicles become weaker, hair grows thinner, shorter, and eventually stops growing altogether. Male Pattern Hair Loss Stages Hair loss in men typically follows a predictable pattern, often described using stages: Early stage: Receding hairline or thinning at the temples Mid stage: Thinning at the crown with visible scalp Advanced stage: Significant recession and reduced density across the scalp Can You Prevent Male Hair Loss? While genetics cannot be changed, the progression of male hair loss can often be slowed or managed with the right approach. Early intervention helps preserve existing hair, improve scalp health, and support stronger regrowth. We believe identifying hair loss early is key because treatments are most effective when follicles are still active, even if hair appears thinner. Our unique prevention techniques focus on: Reducing inflammation in the scalp Supporting healthy follicle function Addressing hormonal and lifestyle contributors Using evidence-based treatments consistently Source link