
Not every man dressed in a red suit in the month December is Santa Claus. And not every patient with a dual diagnosis of lichen planopilaris (LPP) and androgenetic alopecia (AGA) has fibrosing alopecia in a pattern distribution (FAPD).
Over the past few years, I’ve become increasingly concerned (to say it lightly) about a quiet shift in how FAPD is being diagnosed in the world. There is a growing tendency to label patients as having FAPD simply because they carry two diagnoses: lichen planopilaris (LPP) and androgenetic alopecia (AGA).
But this is not what FAPD is. So this trend is wrong. FAPD is not merely the coexistence of LPP and AGA. It is a distinct clinicopathologic entity.
Patients with FAPD typically show:
1) A symmetrical, patterned distribution of hair loss (often central scalp)
2)A presentation that mimics AGA—but behaves differently
3) Loss of vellus hairs with relative preservation of many isolated terminal hairs
4) Subtle but important signs of inflammation, including perifollicular scale or erythema
In contrast, classic LPP more often produces patchy, irregular areas of scarring hair loss.
The introduction of the concept of discordant anisotrichosis by Saber et al in 2026 has been an important step forward.
In typical AGA, hair shaft variability follows a relatively uniform and predictable progression. In FAPD, however, the variability is less than what is expected for the amount of density reduction.
This feature provides a practical clue that something more than AGA is occurring.
FAPD is not common—and it should not become a default label of AGA+LPP. Cases of FAPD have skyrocketed- and many diagnoses are wrong.
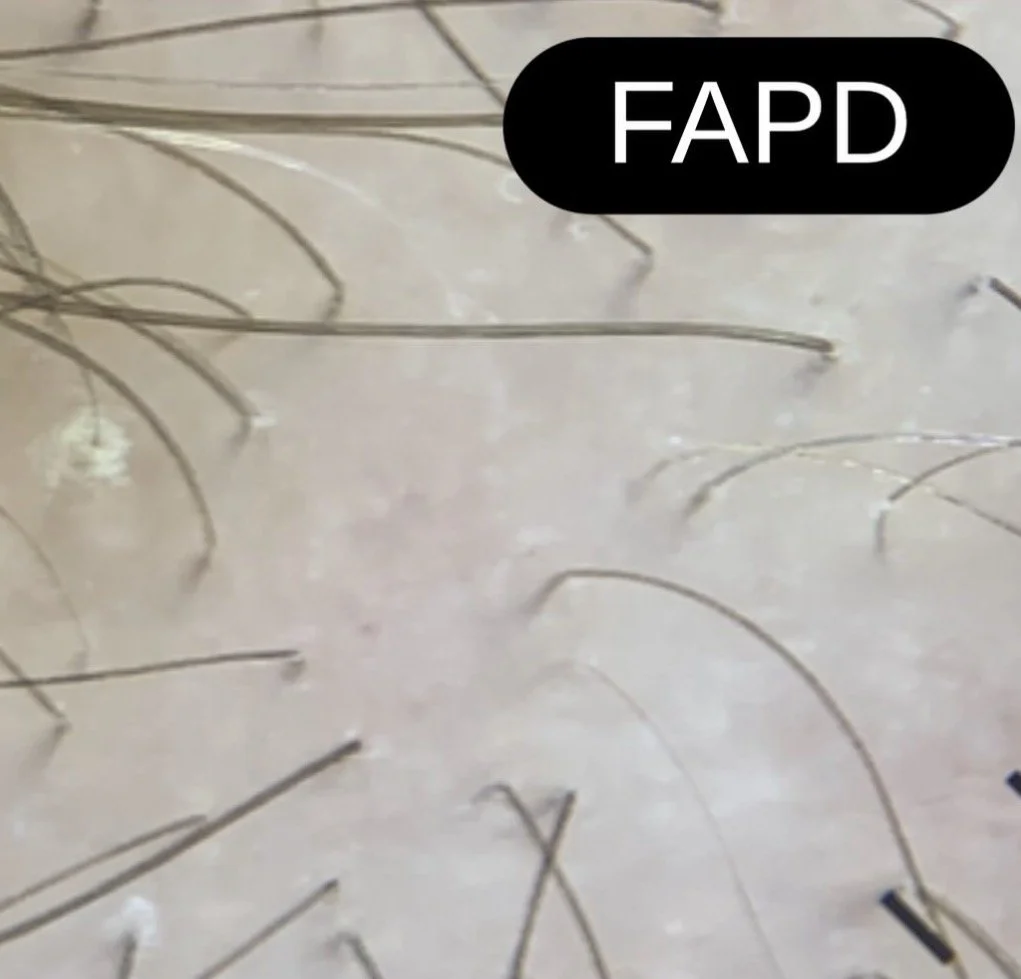
The image shown here highlights some key features of FAPD. There is discordant anisotrichosis. Many follicular units contain single terminal hairs. Vellus hairs are not seen. Subtle perifollicular inflammation and scale can also be appreciated.


