Key takeaways
- Mufemilast 60 mg improved clinical remission rate at 12 weeks, which was maintained through 24 weeks.
- Incidence of adverse events was similar between treatment and placebo groups.
CHICAGO — An investigational small-molecule oral phosphodiesterase-4 inhibitor appeared well-tolerated and maintained clinical remission rates at 24 weeks among adults in China with ulcerative colitis, according to data presented.
The novel drug, mufemilast (Hemay005, Tianjin Hemay), has been approved in China for patients with plaque psoriasis, but does not have FDA approval.

Data derived from Jones CR, et al. Mufemilast (oral pde4 inhibitor) for ulcerative colitis: Open-label extension results at 24 weeks from a multicenter, randomized, double-blind, placebo-controlled parallel group induction phase II clinical trial. Presented at: Digestive Disease Week; May 2-5, 2026; Chicago.
Results from a recent trial were presented at Digestive Disease Week.
“When looking at this drug, there are some preclinical data that are quite interesting,” presenting author Laurent Peyrin-Biroulet, MD, PhD, head of the IBD unit at Nancy University Hospital in France, told attendees at the meeting. “On top of [an impact on] inflammation, there is also an impact on fibrosis.”
Peyrin-Biroulet and colleagues investigated use of mufemilast in UC by conducting a phase 2, double-blind, placebo-controlled trial of 92 patients with moderate to severe disease. Patients needed a modified Mayo score of 4 to 9, an endoscopy score at least 2, and inadequate/failed response or intolerance to conventional therapy or biologics.
Participants were randomly assigned to 45 mg mufemilast (n = 31), 60 mg mufemilast (n = 30) or placebo (n = 31) twice daily for 12 weeks, after which all groups switched to 60 mg mufemilast for an additional 12 weeks.
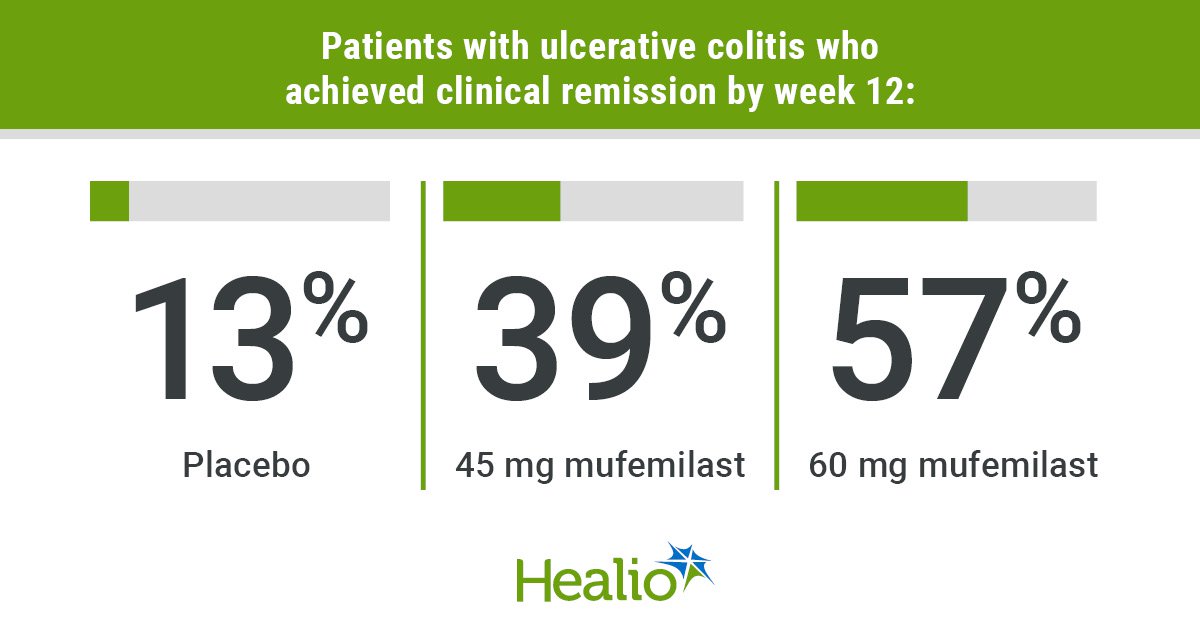
Clinical remission rate at week 12 served as the primary endpoint. Secondary endpoints included clinical remission rate at week 24 and clinical response rate at weeks 12 and 24.
Analysis included 70 patients who received 60 mg mufemilast in the open treatment period.
Results showed clinical remission rates improved from 13% at 12 weeks to 75% at 24 weeks in the group originally assigned placebo, and from 39% to 62% in the group that switched from 45 mg to 60 mg. Remission rates remained steady in the group assigned 60 mg mufemilast for the entire 24-week period (57% to 52%).
Researchers also reported increases in clinical response from week 12 to 24 for the groups originally assigned placebo (42% to 81%) and 45 mg mufemilast (87% to 90%), as well as in endoscopic improvement (placebo: 16% to 75%; 45 mg: 42% to 66%).
The group assigned 60 mg achieved an 80% clinical response rate at 12 weeks, which dropped slightly to 72% by week 24, and also demonstrated endoscopic improvement (week 12: 67%; week 24: 64%).
No significant differences were observed between responses of biologic-naive and biologic-exposed patients.
Two adverse events and one severe adverse event — associated with preexisting thrombophlebitis — in the 60 mg group led to trial discontinuation.
Incidence of adverse events was comparable between the treatment and placebo groups and included headache, dizziness and nausea.
The incidence of headache, which ranged from 9.68% in the placebo and 45 mg groups to 10% in the 60 mg group during the 12-week treatment period, dropped to 2.86% in the open treatment period.
Peyrin-Biroulet noted that tuberculosis, which is endemic in China, was an additional safety outcome in the study.
“Despite having 17 TB-positive patients receiving mufemilast, no reactivation of TB was observed,” he said.
“[Mufemilast] has improved efficacy, significant treatment effect and dose response — which is something that is very important,” Peyrin-Biroulet said.
Sources/Disclosures
Source:
Jones CR, et al. Mufemilast (oral pde4 inhibitor) for ulcerative colitis: Open-label extension results at 24 weeks from a multicenter, randomized, double-blind, placebo-controlled parallel group induction phase II clinical trial. Presented at: Digestive Disease Week; May 2-5, 2026; Chicago.
Disclosures:
Healio was unable to confirm relevant financial disclosures at time of publication.
Ask a clinical question and tap into Healio AI’s knowledge base.
- PubMed, enrolling/recruiting trials, guidelines
- Clinical Guidance, Healio CME, FDA news
- Healio’s exclusive daily news coverage of clinical data