Key takeaways:
- About a third of patients do not have a biomarker used to track treatment progress in pancreatic cancer.
- An AI biomarker derived from routinely collected data predicted treatment completion and survival.
Approximately a third of patients with pancreatic ductal adenocarcinoma do not have elevated or detectable levels of a biomarker commonly used to measure response to therapy.
An AI tumor marker derived from routinely collected data could provide prognostic information on treatment completion and survival similar to that seen in patients who have measurable cancer antigen 19-9 (CA19-9).

Data derived from Thalji SZ, et al. JAMA Surg. 2026;doi:10.1001/jamasurg.2026.0291.

Anai N. Kothari
“This behaves just like CA19-9 does clinically,” Anai N. Kothari, MD, MS, assistant professor of surgical oncology at Medical College of Wisconsin, told Healio. “It tracks response, predicts outcomes and can help guide treatment decisions. This really is a step forward using AI, not just to predict outcomes, but to fill in some critical gaps in clinical care using data we already have.”
‘A big gap’
Pancreatic ductal adenocarcinoma (PDAC) tumors can exhibit significant changes on imaging, so clinicians use biomarker CA19-9, a serum blood value, to measure response to therapy and make prognostic assessments, according to study background.
However, about 30% of patients with PDAC do not produce elevated levels of CA19-9, including 10% who do not have any detectable CA19-9.
“There’s no high-quality biomarker in that patient population to follow,” Kothari said. “Instead, [clinicians use] a lot of intermittent screening tests, imaging that ends up being costly and challenging for the patients to do. They may miss an opportunity to change treatment in someone who’s not responding. This is a big gap that needed to be filled.”
Kothari and colleagues investigated whether AI could use other common laboratory data routinely collected along with CA19-9 to find a surrogate biomarker, which they called electronic CA19-9 (e19-9).
They trained the model on 3,239 patients with PDAC and elevated C19-9. The cohort had a combined 21,555 unique CA19-9 values.
Researchers then conducted external validation on 4,384 similar patients with 16,487 unique CA19-9 values.
Finally, they tested the model on 121 patients with localized PDAC (median age, 65 years; interquartile range, 14; 51% men; 89% white) who did not have elevated CA19-9 (less than 35 U/mL).
Completion of all neoadjuvant treatment and surgery, metastatic progression and OS served as primary endpoints.
‘Highly usable tool’
Overall, 77% of patients in the test cohort completed neoadjuvant therapy, including surgery.
Individuals who finished treatment had similar e19-9 values before therapy as those who did not complete treatment (median, 121 vs. 134.1).
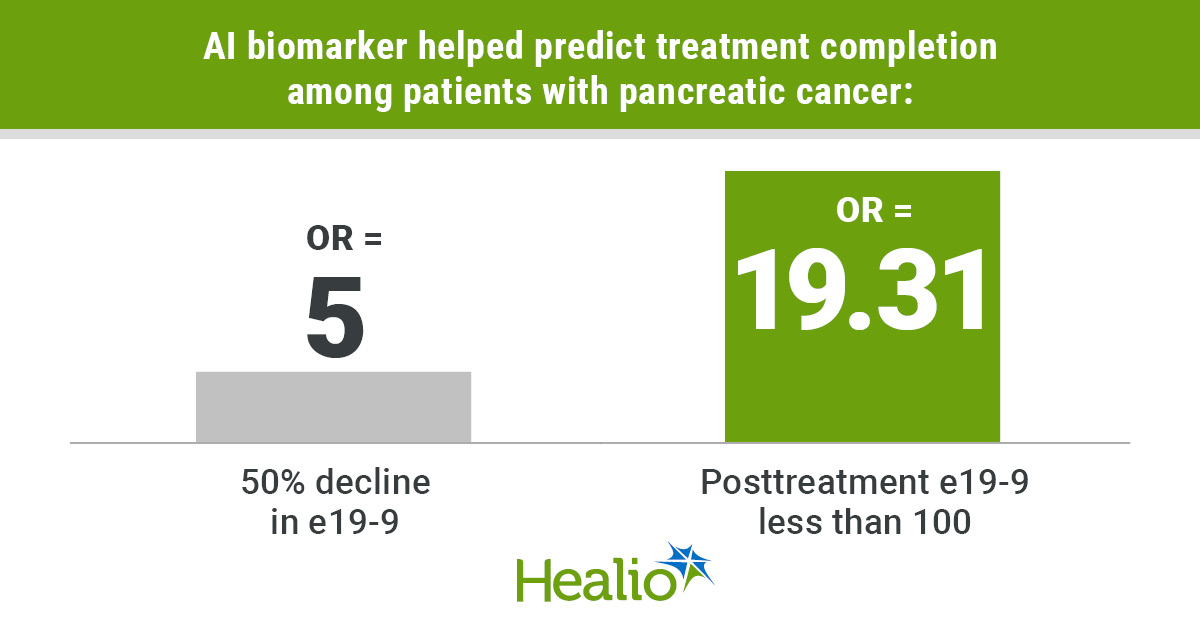
Kothari and colleagues found patients who had at least a 50% decline in e19-9 during treatment had a significantly higher likelihood of finishing (OR = 5; 95% CI, 1.6-15.66).
Additionally, patients who had posttreatment e19-9 levels less than 100 had nearly 20 times the likelihood of completing therapy, including surgery (OR = 19.31; 95% CI, 5.8-64.26).
Metastatic progression occurred significantly less in patients who had any decline in e19-9 (47% vs. 80%; P = .01), those who had a 50% decrease (24% vs. 56%; P = .01), and those with levels less than 100 (29% vs. 80%; P < .001).
OS significantly increased among patients who had any decline in e19-9 (median, 49 months vs. 22 months; P = .03), those with a 50% reduction (median, 53 months vs. 32 months; P = .007), and those with posttreatment levels less than 100 (median, 60 months vs. 16 months; P < .001).
E19-9 less than 100 had a significant association with improved OS (HR = 0.49; 95% CI, 0.25-0.97).
“This is a highly usable tool, and it sets the stage for a lot more innovation and impact by using AI the right and responsible way,” Kothari said.
“Before, for this 30% of patients who have pancreas cancer, we didn’t have a reliable way of making these estimates over time. Now, the data show we have a biomarker for that 30%. We have something that can guide treatment decision-making, to look at things over the course of their therapy, and to be able to give them some idea of the probability that they would make it to surgery, or what their survival could look like.”
Researchers acknowledged study limitations, including e19-9 being based on a predictive model.
Kothari noted the importance of further prospective analysis at different institutions.
He also highlighted the impact this could have on other malignancies.
“Why stop at pancreas cancer?” he asked. “We know that tumor biomarkers are important parts of other cancers, and similar to the problem in pancreas cancer, there’s a subset of patients who don’t have a meaningful ability to use that biomarker. There are other populations we can help with this same methodology. The key is that we’re not drawing any new information, new labs. We’re just using the data we already have to be able to provide this information.”
This is the benefit AI can provide.
“I’ve been studying artificial intelligence for over a decade,” Kothari said. “There’s always this promise that AI was going to identify information that the human eye could not see. For an individual patient with cancer, we now gather up to a million data points as part of their treatment. We can use AI to see patterns, then augment that with our human expertise to improve not just cancer outcomes, but health outcomes overall. Instead of treating everyone exactly the same, we really are homing in on what’s personal and unique about that individual.”
For more information:
Anai N. Kothari, MD, MS, can be reached at akothari@mcw.edu.
Sources/Disclosures
Source:
Thalji SZ, et al. JAMA Surg. 2026;doi:10.1001/jamasurg.2026.0291.
Disclosures:
Kothari reports grants from Amazon Web Services and Triomics, nonfinancial support from Wisconsin Health Informational Organization and a pending patent application (PCT/US2023/074508). Please see the study for all other authors’ relevant financial disclosures.
Ask a clinical question and tap into Healio AI’s knowledge base.
- PubMed, enrolling/recruiting trials, guidelines
- Clinical Guidance, Healio CME, FDA news
- Healio’s exclusive daily news coverage of clinical data