Editorials
Editorials
This month’s Healio Exclusive in Healio Gastroenterology poses a highly topical question.
GLP-1 receptor agonists have revolutionized the treatment of obesity and related conditions, including type 2 diabetes, major adverse cardiovascular events, obstructive sleep apnea, metabolic dysfunction-associated steatotic liver disease, osteoarthritis and polycystic ovarian syndrome.

The benefits of this drug class seem to far outweigh adverse events, which are often gastrointestinal. For some patients, including those with MASLD, gastroesophageal reflux disease or inflammatory bowel disease, there is evidence that these drugs may provide benefit. I personally have witnessed significant improvement in gastrointestinal symptoms for some of my patients with Crohn’s disease, ulcerative colitis and ileoanal pouch dysfunction.
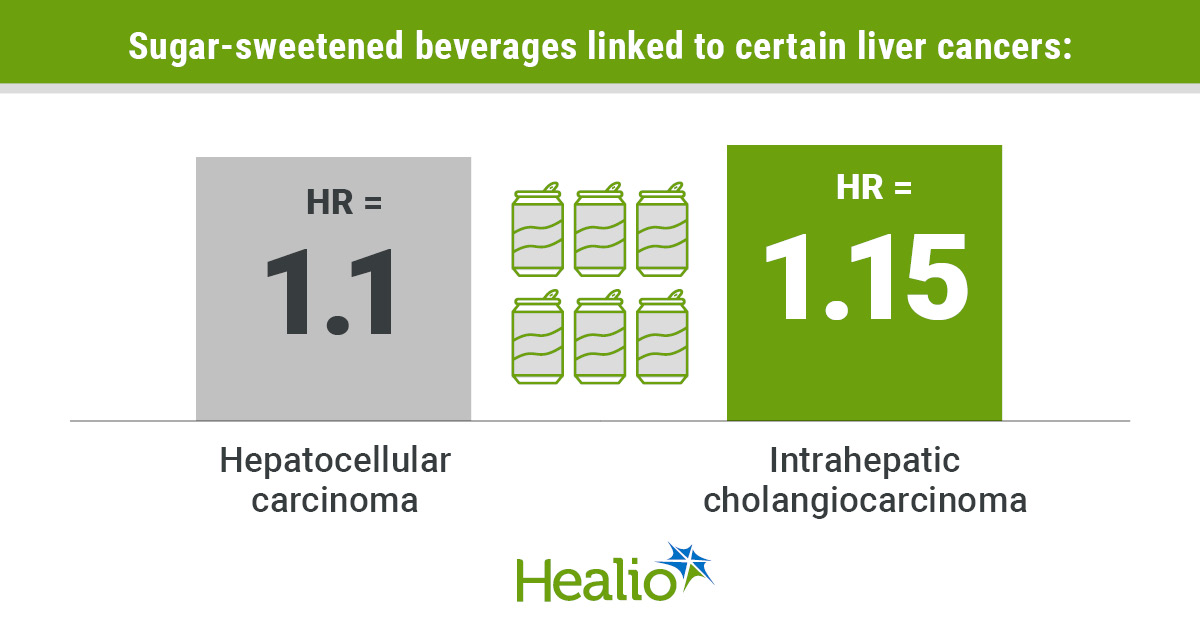
Furthermore, given the association between BMI and risk for gastrointestinal cancers, use of GLP-1s may prevent these malignancies. This raises the question: Should gastroenterologists prescribe these drugs as well?
GLP-1s often seem to be under the purview of endocrinologists, weight management specialists or primary care providers. In one camp, we hear from gastroenterologists who subspecialize in obesity and feel we should fully embrace this drug class and be comfortable prescribing them.
However, we also hear concerns about how GLP-1s are being marketed directly to patients through online health platforms, leading to little or no oversight of the prescription. One could argue this is a sign of primary care provider shortage and another reason for gastroenterologists to take ownership of prescribing GLP-1s. Given the broad number of indications for these drugs, it may be best for the primary care provider to “be the quarterback” and handle the prescribing.
Certainly, gastroenterologists should embrace drugs such as tirzepatide and semaglutide in the sense that they should encourage patients with overweight or obesity to try them when the question is raised. As mentioned by Michael Camilleri, MD, DSc, in the cover story, use of GLP-1s fits nicely within the spectrum of treatments that should be offered to these patients after diet and lifestyle modifications but before endoscopic or surgical bariatric procedures.
We also should be familiar with and comfortable discussing potential side effects of these medications, which include nausea, vomiting, diarrhea, constipation, indigestion, abdominal pain, fatigue and belching. We can talk patients through some of these side effects and reassure them that generally, they ease with time. We also should be aware of less common and more severe side effects such as biliary problems, pancreatitis and allergic reactions.
Ultimately, the decision for a gastroenterologist to prescribe GLP-1s is a personal one and will depend on their patients and the availability of primary care providers who are comfortable with this class of drugs.
Further research into the effect of the use of this drug class on gastrointestinal cancer prevention is warranted, too.
For more information:
Edward V. Loftus Jr., MD, is the Maxine and Jack Zarrow Family Professor of Gastroenterology at the Mayo Clinic and chief medical editor of Healio Gastroenterology. He can be reached at loftus.edward@mayo.edu.
Editorials
Sources/Disclosures
Source:
Expert submission
Disclosures:
Loftus reports consulting for AbbVie, Alvotech, Amgen, Boehringer Ingelheim, Bristol Myers Squibb, Celltrion Healthcare, Eli Lilly & Co., Fresenius Kabi, Gilead Sciences, Janssen and Takeda Pharmaceuticals; and receiving research support from AbbVie, Bristol Myers Squibb, Celgene/Receptos, Gilead, Janssen and Takeda.
Ask a clinical question and tap into Healio AI’s knowledge base.
- PubMed, enrolling/recruiting trials, guidelines
- Clinical Guidance, Healio CME, FDA news
- Healio’s exclusive daily news coverage of clinical data