Key takeaways:
- A computer-aided detection system improved adenoma detection rate and had higher adenomas per colonoscopy among FIT-positive patients.
- The improvement was mostly driven by diminutive adenoma detection.
AI-assisted colonoscopy could detect diminutive adenomas at higher rates than standard colonoscopy, which could be beneficial to populations at high risk for colorectal cancer.
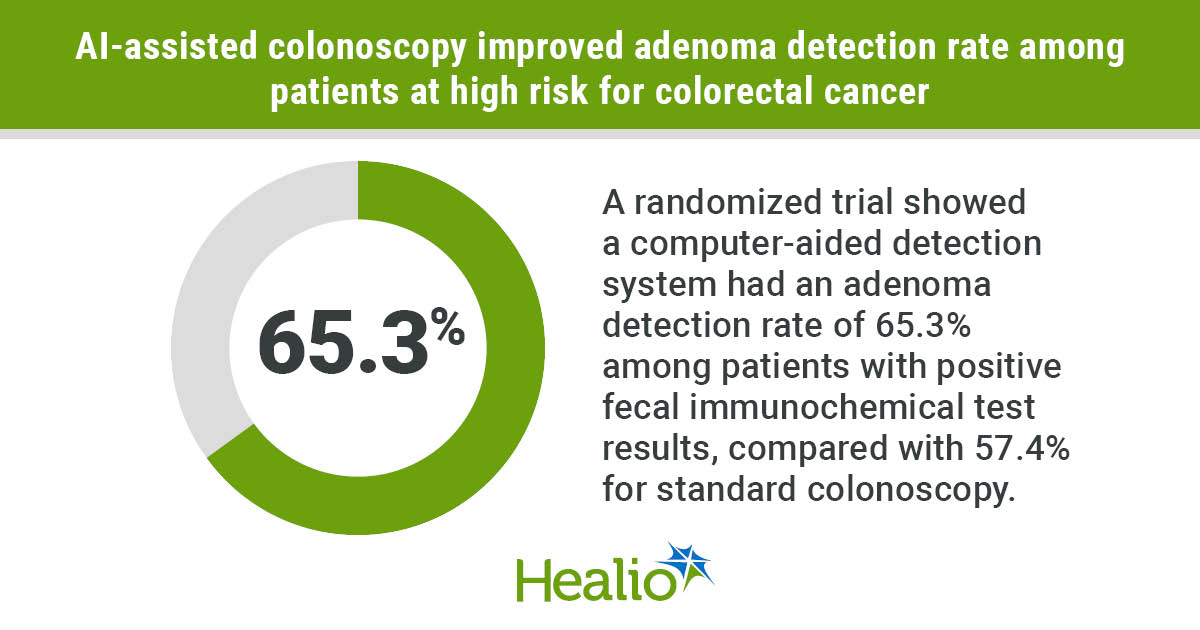
A randomized trial of more than 1,300 individuals in Taiwan showed computer-aided detection (CAD) was noninferior to standard colonoscopy for adenoma detection in the general population, but had a 39% higher likelihood of detecting adenomas among patients with positive fecal immunochemical test (FIT) results.

Data derived from Hsu WF, et al. JAMA Netw Open. 2026;doi:10.1001/jamanetworkopen.2026.4881.
“CAD should be strategically deployed as a precision tool for high-risk cohorts and as a quality-standardization asset within organized screening programs,” Han-Mo Chiu, MD, PhD, attending physician at National Taiwan University Hospital, told Healio.
“In FIT-positive patients, more is not just more. Finding more diminutive adenomas is clinically vital. Because these small lesions in high-risk patients have a higher propensity for advanced histology like [high-grade dysplasia (HGD)], using AI to maximize their detection directly addresses the risk of interval cancers that might otherwise be overlooked in a manual exam. Crucially, this enhanced detection is achieved without over-resection.”
‘A unique high-risk cohort’
Adenoma detection rate has a significant association with interval colorectal cancer, according to study background.
Prior studies have shown every 1% increase in detection decreases risk for colorectal cancer 3%, but up to 26% of adenomas and 27% of serrated polyps are missed on standard colonoscopy, most of which are classified as diminutive ( 5 mm) or small (6-9 mm).
CAD has been shown to increase detection of smaller adenomas.
“A major critique is that CAD primarily increases the detection of adenomas less than 1 cm, which some argue may have limited clinical impact in the general population,” Chiu said. “However, we recognized that FIT-positive individuals represent a unique high-risk cohort. They tend to have a higher multiplicity of adenomas, and importantly, even adenomas smaller than 1 cm in this population carry a substantially higher likelihood of advanced histology, such as HGD.
“Our previous study in Taiwan comparing adenomas detected in FIT-positive individuals with those identified in the general population undergoing direct colonoscopy demonstrated that the former have a significantly higher risk of HGD and invasive cancer, even within the same size category of less than 1 cm. This raises the question of whether the common criticism — that CAD mainly increases detection of small adenomas and therefore has limited impact on future colorectal cancer risk — is applicable in the FIT-screening setting.”
Chiu and colleagues conducted a multicenter trial in Taiwan to investigate.
They randomly assigned 1,356 adults aged 40 to 79 years (mean age, 60 years; standard deviation, 9.4; 50% women) undergoing colonoscopy for positive FIT results, gastrointestinal symptoms, screening or surveillance for a history of polyps, to receive either CAD-assisted (n = 675) or standard colonoscopy (n = 681).
Adenoma detection rate served as the primary endpoint. Researchers defined detection rate as the proportion of patients who had at least one histologically confirmed adenoma.
Adenomas per colonoscopy, postpolypectomy surveillance intervals, and sessile serrated lesion detection rate served as secondary endpoints.
‘Critical finding’
Overall, researchers observed noninferiority in adenoma detection rate between CAD (58.5%) and standard colonoscopy (53.1%; P = .01), but the difference did not reach statistical significance (P = .05).
However, among patients with positive FIT results, the CAD cohort had a significantly higher adenoma detection rate (65.3% vs. 57.4%; adjusted OR = 1.39; 95% CI, 1.05-1.86).
“This is a critical finding,” Chiu said. “The AI’s ability to detect more of these subcentimeter adenomas in this trial will hopefully translate into a highly meaningful clinical benefit for this specific group.”
CAD helped identify significantly more adenomas per colonoscopy overall (mean, 1.41 vs. 1.2; P = .01) and in the FIT subgroup (mean, 1.64 vs. 1.39; P = .01), the difference stemming from detection of diminutive adenomas.
The CAD group also had significantly more polyps per colonoscopy (mean, 1.97 vs. 1.71; P = .005).
The CAD and standard colonoscopy groups had similar advanced adenomas per colonoscopy, nonneoplastic polypectomy rates, and sessile serrated lesion detection rates.
However, withdrawal time was significantly longer with CAD than standard colonoscopy (mean, 9.14 minutes vs. 8.32 minutes; P < .001).
Patients who underwent CAD-assisted colonoscopy had a significantly higher likelihood of being assigned to U.S. Multi-Society Task Force intensive surveillance of 3 to 5 years (10.4% vs. 7.2%; aOR = 1.5; 95% CI, 1.01-2.21). Patients in the FIT subgroup had even greater odds (13.2% vs. 7.3%; aOR = 1.94; 95% CI, 1.22-3.09).
“What surprised us the most was how the AI acted as a great equalizer among physicians,” Chiu said. “The benefit of CAD was most pronounced among junior endoscopists, significantly improving their performance, while senior experts saw numerical, but nonsignificant, gains. Furthermore, we were pleased to see that CAD did not increase the nonneoplastic polypectomy rate. This means the AI did not cause our endoscopists to over-resect normal tissue, proving that clinical judgment remained intact alongside the AI assistance.”
Researchers acknowledged study limitations, including use of a single CAD system and not being able to blind endoscopists in the study arm.
“I would like to emphasize the rigorous, high-ceiling setting of our trial,” Chiu said. “We conducted this study across centers where the baseline adenoma detection rate was already exceptionally high — over 50% for all indications of colonoscopy. Demonstrating that AI can still provide measurable clinical benefits in such an optimized environment — specifically by catching high-risk subcentimeter lesions in FIT-positive patients — proves that this technology is not just a crutch for low-performing centers. It is a tool that pushes the boundaries of excellence.”
‘Establish clear criteria’
Chiu described three key components of future research.
The first involves longitudinal follow-up. “Does the removal of these specific AI-detected lesions effectively reduce the long-term incidence and mortality of postcolonoscopy colorectal cancer?” he asked. “We need tracking data to definitively confirm that increased detection translates to enhanced prevention.”
He also anticipated that, “although we were not able to demonstrate the superiority of AI in detecting HGD in adenomas smaller than 1cm in this trial — which would require a remarkably larger sample size — it would be expected to detect more such lesions if it is used across several tens of thousands of colonoscopies performed in our large-scale FIT screening setting.”
The following step involves health economics.
“Because CAD shifts more patients into intensive 3-to-5-year surveillance intervals, we must conduct rigorous cost-effectiveness analyses,” Chiu said. “We need to determine if the financial and operational burden of these additional surveillance colonoscopies is justified by the downstream clinical savings of preventing advanced cancers.”
Lastly, Chiu emphasized the importance of policy integration and updated guidelines.
“We are actively looking at how to incorporate these evidence-based findings into updated guidelines of the Taiwan Colorectal Cancer Screening Program,” he said. “We must establish clear criteria for when and for whom AI should be deployed — such as prioritizing its use for FIT-positive cohorts — to optimize both patient outcomes and the sustainability of the health care system.”
In an accompanying editorial in JAMA Network Open, Masashi Misawa, MD, PhD, associate professor of gastroenterology at Showa Medical University in Japan, and colleagues described the need for “cautious interpretation” of the results, noting the “exploratory” nature of the FIT-positive subgroup analysis.
“The evidence that CAD improves [adenoma detection rate] is well established,” they wrote. “What remains unproven is whether this improvement reduces [colorectal cancer] incidence — the outcome that ultimately matters. Future trials should move beyond [adenoma detection rate] as the primary endpoint and assess [postcolonoscopy colorectal cancer] incidence, advanced neoplasia over long-term follow-up, and cost-effectiveness in organized screening programs.”
For more information:
Han-Mo Chiu, MD, PhD, can be reached at hanmochiu@ntu.edu.tw.
Sources/Disclosures
Source:
Hsu WF, et al. JAMA Netw Open. 2026;doi:10.1001/jamanetworkopen.2026.4881.
Reference:
Disclosures:
Chiu reports grant support from National Science and Technology Council. The other authors report no relevant financial disclosures. Misawa reports personal fees from Olympus Corp. and Cybernet Systems. Please see the study for all other authors’ relevant financial disclosures.
Ask a clinical question and tap into Healio AI’s knowledge base.
- PubMed, enrolling/recruiting trials, guidelines
- Clinical Guidance, Healio CME, FDA news
- Healio’s exclusive daily news coverage of clinical data