
I originally wrote this post on the arrector pili muscle (APM) and its connection to androgenetic alopecia (male pattern hair loss) in 2017. This was followed by important updates in 2020 and 2022. And now we have yet another major update again in 2026. Note that this post is in chronological order, so the latest update is at the bottom.
Jan 10, 2017
Androgenetic Alopecia: New insights into the role of the Arrector Pili Muscle
Several weeks ago, the arrector pili muscle got significant coverage in a few newspapers around the world. Famed Australian dermatologist Dr. Rodney Sinclair co-authored an important paper titled “The arrector pili muscle, the bridge between the follicular stem cell niche and the interfollicular epidermis” that was just published this month.
Dr. Sinclair has been involved in this area of hair loss research for a few years. See his 2014 paper titled: Beyond goosebumps: Does the arrector pili muscle have a role in hair loss? Also see the very interesting new insights on the APM section of his website. Australian newspapers were especially interested in this latest study and its findings as evidenced by articles such as this one and this one.
The Arrector Pili Muscle
Arrector pili muscles are small muscles attached to individual human hair follicles on both the scalp as well as body (so we have millions of these muscles throughout our bodies). Contraction of these muscles causes hairs to stand up, a phenomenon that is known as goosebumps. Therefore, the musculus arrector pili is often referred to as the goosebump muscle.
Every hair root is connected to the arrector pili. This smooth muscle contracts in response to signals from the “fight or flight” sympathetic nervous system.
Arrector Pili Muscle Degeneration and Hair Loss
In recent years, a few studies have come out that suggest a possible connection between the arrector pili muscle degenerating (where it gets replaced by fat) and hair loss due to the subsequent disconnection between various hair follicle stem cell populations. It is possible that an intact APM plays a crucial role in the maintenance of follicular integrity and stability. However, there are many uncertainties about this theory that I discuss in the next section.
It seems that while in alopecia areata (AA) patients the arrector pili muscle remains intact, this is not true in androgenetic alopecia (AGA) patients. So this could be why it is much easier to grow back hair for people with AA compared to people with AGA. Unfortunately, over 95 percent of balding men suffer from AGA.
Of note, the rate at which the arrector pili muscle degenerates and gets replaced by fat varies substantially between patients and between individual hairs on the same scalp. Some miniaturized vellus hairs in balding regions might even never lose most of their arrector pili muscle connection.
My Thoughts and Points of Contention
- According to Dr. Sinclair’s own quote from a past paper, “It remains unclear whether arrector pili muscle regression is a cause or effect of permanent follicle miniaturization“. I think this is the crux of the issue surrounding this theory/hypothesis.
- I am curious why hair that is transplanted from the back of a person’s scalp to the front grows so well if the arrector pili muscles in front have been destroyed? Surely the transplanted hair cannot just automatically regenerate the APM?
- Related to the above, an important Japanese study from 2012 concludes that correctly transplanted hair can re-enable “connectivity and cooperation” with the arrector pili muscle and nerve system. In effect, it might be very possible to reactivate or regenerate the APM.
- In Dr. Tsuji and his team’s groundbreaking technology “the transplanted primordium also forms connections with surrounding tissues (arrector pili muscle and nerves) and repeats normal hair cycles”.
- There are 100s of online anecdotal reports with before and after photos of people re-growing long-lost hair in bald scalps. Miracle results are especially common in people undergoing male-to-female transition regimens. You can also find many reports of surprising hair regrowth in many old men who recently started taking dutasteride for enlarged prostate issues. And the Reddit result logs from people taking oral minoxidil are sometimes spectacular. Maybe they regenerated their arrector pili muscles; or maybe those muscles always remained intact in spite of severe AGA; or maybe one can regenerate hair without the need for having any intact arrector pili muscles?
- It is unclear when exactly we have a point of no return where the arrector pili muscle is largely or entirely replaced by fat and hair stops growing (either as a cause or effect). It seems like there is significant variation depending on the person and hair follicle. In many cases, the APM might not be entirely degenerated and replaced by adipose tissue even in areas of the scalp where one has been bald for several decades. In such cases, subsequent hair and muscle regeneration could then be possible via something like dutasteride or finasteride.
Update: August 7, 2020
Goosebumps, the Sympathetic Nervous System and Hair Growth
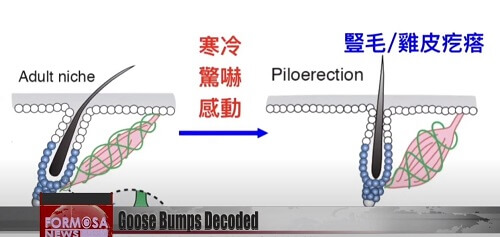
Yesterday, Taiwanese and US researchers published an important paper titled: “Cell Types Promoting Goosebumps Form a Niche to Regulate Hair Follicle Stem Cells.” The work was led by Dr. Sung-Jan Lin of National Taiwan University, in collaboration with researchers from Harvard University (US).
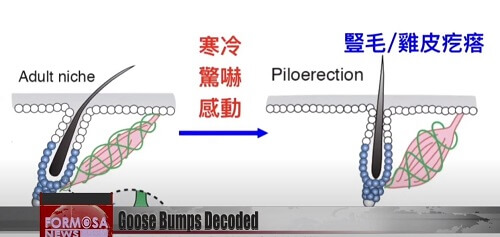
The scientists made some important discoveries in relation to the arrector pili muscle and the sympathetic nervous system. The APM maintains sympathetic innervation to hair follicle stem cells. (HFSCs) The sympathetic nerve activates HFSCs via synapse-like contacts and norepinephrine. An important quote:
“APMs are often lost in the scalp skin of people with androgenetic alopecia. It is possible that in such skin, loss of APMs leads to the loss of sympathetic nerves, making HFSCs more difficult to activate. Our results also suggest the potential of using selective β2 agonists to promote HFSC activation.”
Lin’s team found that the biological mechanism behind baldness in men is closely connected to the sympathetic nervous system. Hair follicle stem cells activate after receiving signals via what are known as ADRB2 receptors. Based on these findings, the researchers hope to develop small molecule drugs that can activate ADRB2 receptors as a means of regenerating hair.
Goose bumps are a sympathetic nerve response involving the contraction of tiny muscles all over our bodies. These arrector pili muscles causes hair to stand up straight on the skin when we are fearful and under threat. The scientists aim to ultimately control the muscle-nerve system that drives hair regeneration. A video of these findings is embedded below. It is quite something to see Dr. Lin Sung-jan being mobbed by the media.
Update: September 28, 2022
The Irreversible Destruction of the Arrector Pili Muscle in Bald Men
Recently, I discovered a 2021 video in which the semi-retired dermatologist Dr. Andrew Messenger of the UK makes some important claims. He thinks that current hair loss treatments mainly impact the hair cycle. They do not reverse miniaturization, and he presents proof of this phenomenon.
Moreover, he theorizes that the structural changes in miniaturized hair follicles are perhaps more profound that previously foreseen. In particular, the irreversible destruction of the arrector pili muscle and subsequent fat infiltration. He presents an image from Dr. Rodney Sinclair’s 2014 paper on this subject, which I discussed in one of my past updates further below.
However, I am skeptical about the irreversibility of hair regrowth once the APM is beyond repair. See the “My Thoughts and Points of Contention” section that I wrote in the original version of this post further above.
It seems like Dr. Ralf Paus in the second half of the above video is also optimistic about the potential reversal of miniaturized hairs via a number of treatments.
I am especially curious as to how hair transplants on people with extensive Norwood 5-6 level balding work so well (since arrector pili muscles throughout their scalp are destroyed). Even body hair to scalp transplants often work well (especially beard hair). Can body hair follicles that are moved to the scalp help reinvigorate dead arrector pili muscles? Or can you actually move arrector pili muscles that are attached to body hair to the scalp?
Also of interest, as I mentioned earlier, there are quite a few spectacular male-to-female transition hair growth results that are solely credited to medications such as dutasteride, finasteride, minoxidil, spironolactone and estrogen.
Update: May 31, 2026
Detachment of the Arrector Pili Muscle Precedes Miniaturization in Androgenetic Alopecia?
At the just ended 14th World Congress for Hair Research, I noticed there was a presentation in relation to the arrector pili muscle. It was titled:
“Detachment of the arrector pili Muscle from the hair bulge precedes miniaturization in androgenetic alopecia.”
The person who made this presentation, Michal Kasprzak, works at a Poland-based company named TrichoLab. The company uses the latest AI and 3D imaging technologies for the purposes of scalp hair health diagnosis, hair loss and hair growth monitoring and hair transplant planning.
While browsing their blog, I found a post from April 26, 2026 titled:
“The secret your hair tells before it falls out.”
It is related to the APM and new potentially groundbreaking findings from the analysis of the scalp hair of 79 balding men undergoing hair transplants. Their conclusion:
“We had previously assumed that APM detachment was a consequence of miniaturisation. This finding raises the possibility that miniaturisation could instead be its consequence.”
The researchers used TrichoLab’s leviacam equipment and TrichoLAB 3D Studio scanning technology.
I will not summarize the methodology here as you can read the above linked article. The main item of initial interest to me is that they claim that poor angular alignment of hair follicles on the surface (when exiting the skin) is an indication of the detachment of the APM from the outer root sheath at the follicle bulge in the dermis.
Per the study’s trichoscopy images (and their theory):
- The average hair spread angle with an intact APM is 7.6 degrees.
- The average hair spread angle with a detached APM is 11.4 degrees.
Note that they are claiming that this means a detached APM, but I am not sure if it is necessarily true as yet (see Dr. Cole’s notes at the end of this post).
The conventional assumption in the hair loss field has been that APM detachment happens after a follicle has already miniaturized. But this new research has found misaligned hairs in thick terminal hairs. i.e., a sign of APM detachment in hairs that hadn’t miniaturized yet. Quote:
“The muscle was already letting go before the hair had begun to shrink.”
Far more research needs to be done for this to be proven conclusive. If true, it would really alter the understanding of androgenetic alopecia. Perhaps APM detachment isn’t a consequence of hair loss, but rather, a driver of the process? I am skeptical for now, but am impressed at the unique method of this latest research (when it comes to analyzing hair follicle angles above the skin).
On a related note, this 2024 study from the US connects curly hair follicles with contracted arrector pili muscles. It has some great diagrams.
Addendum
Dr. John Cole has given me some detailed feedback about this in our Whatsapp group and I am pasting some of the more salient points below. He does not believe that one can make such a conclusion from just these current above-the-skin hair follicle images.
- Current imaging technologies such as TrichoLAB and HairMetrix, even when using AI, cannot accurately count individual hairs. TrichoLAB performs reasonably well with follicular unit counts, and both systems can provide useful diameter measurements, but that is very different from accurately identifying individual follicular anatomy.
- The new paper suggests that hair shaft divergence or angular spread may reflect APM detachment. However, hairs do not emerge perpendicular to the scalp, nor do they grow in identical directions within a follicular unit. Natural variation in exit angle is normal. To suggest that current imaging systems can reliably infer APM attachment status from surface hair angles alone requires a level of validation that, in my opinion, has not yet been demonstrated.
- My own view is that androgenetic alopecia is fundamentally a progressive miniaturization process affecting individual follicles. Each follicle occupies its own canal within the scalp. Interestingly, someone recently sent me a very thoughtful paper discussing why individual follicles within the same follicular unit may behave differently. Why some lose pigment, why some miniaturize, and why others persist.
- I have spent more than two decades surgically dissecting and extracting follicular units. When you examine thousands upon thousands of follicular units under magnification, it becomes apparent that individual follicles within the same follicular unit age differently. Some miniaturize, some lose pigment, some disappear entirely, while neighboring follicles remain terminal. The process is highly heterogenous.
- My skepticism is directed primarily at the current ability of imaging systems to reliably infer complex follicular biology from surface observations alone. As you know, there is a tremendous amount of anatomy beneath the skin that neither trichoscopy nor AI can directly visualize.
- The central questions is whether loss of the APM is the primary event driving follicular degeneration or whether it is a secondary consequence of the same biological processes that drive miniaturization. There are many alternative explanations. Chronic inflammation, perifollicular fibrosis, extracellular matrix remodeling, mechanotransduction abnormalities, altered WNT-BPM signaling, YAP/TAZ dysregulation, stem cell dysfunction, and androgen receptor mediated changes could all influence bother the follicle and the arrector pili muscle simultaneously.
- At present, the concept that loss of the APM causes hair loss remains an interesting hypothesis, but it is still a hypothesis. Demonstrating an association is not the same as demonstrating causation. Until there is evidence showing that selective loss of the APM initiates follicular miniaturization in otherwise healthy follicles, we should be cautious about assigning it a primary pathogenic role.
Also check out the interesting replies to my Tweet about this news.

