
Key takeaways:
- ddPCR analysis at diagnosis and after treatment detected KRAS-mutant circulating tumor DNA more frequently than standard testing.
- The approach could allow for intervention before recurrence is clinically visible.
A highly sensitive blood test can detect signs of pancreatic cancer that standard methods often miss, according to results of a prospective cohort study.
Digital droplet polymerase chain reaction (ddPCR) analysis performed upon diagnosis of localized disease detected KRAS-mutant circulating tumor DNA (ctDNA) nearly four times more often than more widely used next-generation sequencing, with results strongly predicting survival.

Administration of ddPCR after chemotherapy or surgery also detected traces of ctDNA with the key genetic mutation at considerably higher rates, suggesting it more effectively identifies patients with residual disease who are at greater risk for recurrence.

Akhil Chawla
“These findings provide important insights into what we are missing with next-generation sequencing — particularly after a patient has been treated,” senior author Akhil Chawla, MD, FACS, clinical associate professor of surgery at Northwestern University Feinberg School of Medicine and complex surgical oncologist at Northwestern Medicine, told Healio. “The goal of getting more patients to cure requires a thoughtful analysis of each individual. It is an obvious hypothesis that, if a patient has a high risk for recurrence based off what we are seeing in their blood and we treat a patient earlier with a targeted treatment, that patient likely will do better.”
Focusing on KRAS
Only 13% of patients with pancreatic ductal adenocarcinoma (PDAC) live 5 years after diagnosis, according to American Cancer Society statistics.
Individuals with localized disease undergo months of chemotherapy and surgery but still often develop recurrence.
Liquid biopsies — blood tests that can be repeated over time — search for traces of DNA that cancer cells shed into the bloodstream, offering an early indication that cancer either is present or may return. However, in many cases, ctDNA levels are low and hard to detect.
RAS mutations, found in more than 90% of pancreatic cancers, have long been known to be a driver of disease development and progression.
Commercially available assays that use next-generation sequencing or digital PCR methods for cancer detection, tumor profiling and therapy selection provide valuable insights, but market forces have driven the technology toward broad panels. In contrast, ddPCR — which often costs less and yields results quicker — analyzes one set of genes at a time.
Studies that Chawla’s group conducted a few years ago using next-generation sequencing panels confirmed KRAS to be the most prognostic mutation in pancreatic cancer.
In their current study, the researchers leveraged that insight to evaluate a ddPCR assay that targets the three most common mutations in the KRAS gene — G12D, G12V and G12R — with about a thousand times more sensitivity than more commonly used broader testing approaches.
The analysis included 106 patients with localized PDAC who were undergoing neoadjuvant chemotherapy across multiple Northwestern Medicine sites as part of a larger clinical trial.
Investigators collected blood samples at multiple time points — at diagnosis, after chemotherapy and after surgery — and performed ddPCR and next-generation sequencing on all samples to assess for KRAS-mutant ctDNA.
A ‘hidden group’
At diagnosis, ddPCR detected KRAS-mutant ctDNA in nearly four times as many patients as next-generation sequencing (64.9% vs. 17.2%).
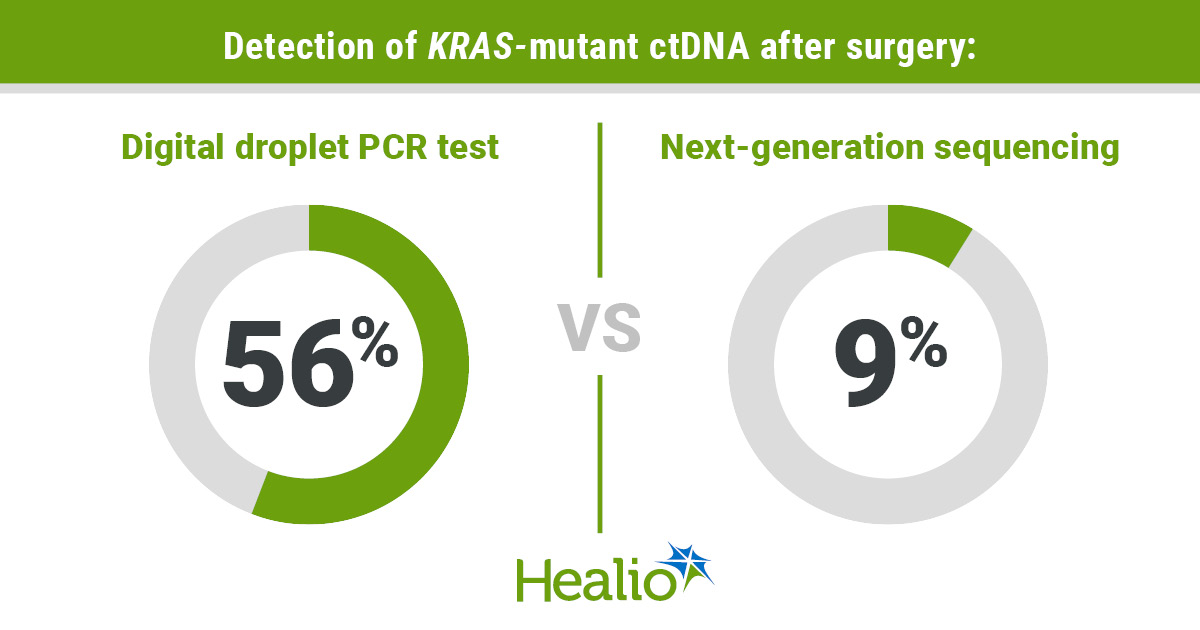
The ddPCR test continued to detect residual cancer more effectively after treatment, identifying KRAS-mutant DNA in 12 times as many patients after chemotherapy (60% vs. 5%) and six times more patients after surgery (56% vs. 9%).
“All of these time points are informative but the diagnosis time point has been shown in our studies to be most prognostic, indicating how a patient will do with subsequent neoadjuvant chemotherapy and surgery,” Chawla said. “This suggests if they have a KRAS mutation at high levels early in their disease course, they may already have more resistant disease or potentially be a more basal-like subtype. These are the patients who recur early and have worse survival.”
Detection of KRAS-mutant ctDNA appeared predictive for outcomes.
Patients who tested negative on both ddPCR and next-generation sequencing survived a median 40.7 months after diagnosis.
A previously “hidden group” of high-risk patients — those whose cancer had been missed by standard next-generation sequencing but detected by ddPCR — survived a median 26.9 months, Chawla said.
Those who tested positive on both tests survived a median 10.9 months (P < .001 for comparison).
The high sensitivity of ddPCR allows it to do more than show “presence or absence” of ctDNA by offering valuable insights into tumor mutational burden, Chawla said.
A fundamental change
Earlier this spring, results from the randomized phase 3 RASolute 302 trial showed the oral pan-RAS inhibitor daraxonrasib (RMC-6236, Revolution Medicines) doubled survival — from 6.7 months to 13.2 months — compared with standard chemotherapy among patients with previously treated metastatic PDAC.
The investigational agent, which can be used under an FDA-authorized expanded access protocol and is expected to receive agency approval later this year, also improved several other outcomes, including doubling time to deterioration of pain and quality of life.
The findings, which culminate a three-decade commitment to overcome what many in the field had considered an undruggable driver mutation, may lay the foundation for additional therapies or combinations that could lead to longer or deeper responses.
This will make the ability to use a high-sensitivity ddPCR test that tracks the same mutation even more valuable, Chawla said.
In fact, it may “fundamentally change” how high-risk patients are identified and microscopic disease is monitored, he said, increasing the likelihood that clinicians can intervene before recurrence is clinically visible.
“This remains a very challenging disease to treat, but it is an exciting time for pancreatic cancer,” Chawla said. “Hopefully improvements in technology can be leveraged with the advances that have been made scientifically to help us further improve outcomes. Biomarker-directed therapy will be crucial to ensure we are using appropriate treatments earlier to optimize outcomes. If a patient is tolerating daraxonrasib, how long do we continue to treat them? What happens when they develop resistance? These are open-ended questions, and we need high-sensitivity biomarkers to answer them.”
The findings from the ddPCR analysis must be validated in larger, multicenter cohorts before the approach can be broadly adopted, Chawla said.
Plasma banks available through larger multi-institutional trials could represent an opportunity to validate the early data.
Investigators also are looking to partner with commercial entities interested in better understanding how KRAS-targeting treatments work with this biomarker, Chawla said.
Use of the ddPCR approach so far has focused on distinguishing “detection vs. lack of detection,” Chawla said. However, he noted it could potentially be used more like “a continuous variable” in conjunction with other biomarkers such as CA 19-9, a protein in the blood that helps clinicians monitor efficacy of pancreatic cancer treatment.
More work also is necessary to determine if ddPCR should complement rather than replace next-generation sequencing.
“Our publication shows we are missing a lot just by doing next-generation sequencing, but next-generation sequencing does have a capability that ddPCR does not,” Chawla said. “The ability to look at a large panel of genes could help us better understand whether co-occurrence of certain genes — such as KRAS and TP53 — has an impact on phenotype or may harbor additional resistance.”
For more information:
Akhil Chawla, MD, FACS, can be reached at akhil.chawla@northwestern.edu.
Ask a clinical question and tap into Healio AI’s knowledge base.
- PubMed, enrolling/recruiting trials, guidelines
- Clinical Guidance, Healio CME, FDA news
- Healio’s exclusive daily news coverage of clinical data

