What Happens During Your Hair Loss Consultation in Scottsdale A Real Conversation First Your consultation begins with a conversation, and we mean a real one. Your clinician will ask about your health history, lifestyle, stress levels, diet, and any significant life changes that may correlate with your hair loss. We are listening for patterns and clues that go beyond what is visible on the surface, because hair loss is almost always a signal of something happening internally. A Thorough Scalp Analysis Using clinical-grade tools, your clinician will conduct a detailed analysis of your scalp and hair follicles. This allows us to assess follicle health, scalp condition, hair density, and the pattern of loss in a way that a mirror at home simply cannot replicate. This step is foundational to building a plan that targets the right areas with the right treatments. Identifying the Root Cause This is where NHLMA differs from a standard office visit. Rather than prescribing a generic solution based on surface symptoms, we work to identify the underlying cause of your hair loss. This might involve a recommendation for comprehensive lab testing to look at hormones, thyroid function, nutrient levels, inflammation markers, and other systemic contributors that often drive hair loss from within. Understanding the root cause is what allows us to build a plan that produces lasting results rather than temporary improvements. Exploring Your Treatment Options Once your clinician has a clear picture of what is happening and why, they will walk you through the treatment options that are most appropriate for your situation. This is a collaborative conversation. We explain the science behind each option, what the process looks like, the expected timeline for results, and how the treatments work together within a personalized protocol. You will leave knowing exactly what we recommend, why we recommend it, and what you can realistically expect. Source link
Regimen ‘extremely encouraging’ in metastatic pancreatic cancer
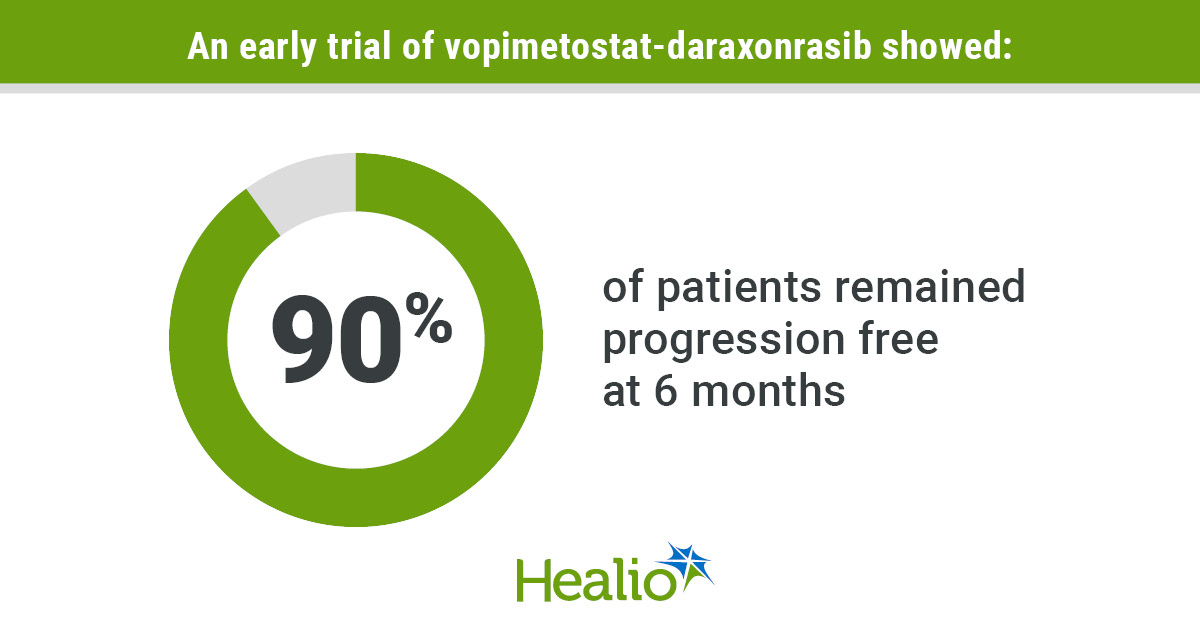
Add topic to email alerts Receive an email when new articles are posted on Please provide your email address to receive an email when new articles are posted on . “ data-action=”subscribe”> Subscribe We were unable to process your request. Please try again later. If you continue to have this issue please contact customerservice@slackinc.com. Back to Healio Key takeaways: 92% of patients responded to second- or third-line treatment with vopimetostat and daraxonrasib, and 90% remained progression free at 6 months. The combination will be advanced into phase 3 development. A two-drug combination exhibited durable clinical benefit as second- or third-line treatment for pancreatic cancer, according to a topline data announcement released by one of the agent’s manufacturers. A vast majority of patients with methylthioadenosine phosphorylase (MTAP)-deleted and RAS-mutant metastatic pancreatic ductal adenocarcinoma (PDAC) responded to treatment with vopimetostat (TNG-462, Tango Therapeutics) and daraxonrasib (RMC-6236, Revolution Medicines), results showed. Most remained progression free at 6 months. The “extremely encouraging early results” support advancing the combination into late-stage development for this patient population, Malte Peters, MD, CEO of Tango Therapeutics, said in a company-issued press release. The design of a randomized phase 3 trial to assess the combination as first-line treatment for MTAP-deleted pancreatic cancer is expected to be finalized in the second half of this year, according to the release. Vopimetostat is an oral PRMT5 inhibitor that targets cancers with MTAP deletions, which occur in up to 15% of cancers and are present in approximately 40% of pancreatic cancers. Daraxonrasib is an oral pan-RAS inhibitor. RAS mutations — found in more than 90% of pancreatic cancers — have long been known to be a driver of disease development and progression. No RAS-targeting therapies are approved for pancreatic cancer. Results of the randomized phase 3 RASolute 302 trial — presented at ASCO Annual Meeting — showed daraxonrasib doubled OS and PFS and tripled objective response compared with chemotherapy for patients with previously treated metastatic PDAC, establishing it as a new standard in this setting. Regulatory approval is expected later this year. A phase 1/phase 2 trial evaluated two combinations for patients with MTAP-deleted and RAS-mutant metastatic PDAC or non-small cell lung cancer, another malignancy in which RAS mutations are common. As of late May, 20 patients with PDAC — 70% of whom had liver metastases — and five with NSCLC had received 200 mg or 250 mg once-daily vopimetostat in combination with 100 mg daraxonrasib daily. At data cutoff, 12 patients with PDAC and three with NSCLC had at least 14 weeks of follow-up and could be evaluated for response. Eleven of 12 (92%) patients with PDAC achieved objective response — with nine responses confirmed — and 90% of patients remained progression free at 6 months. Researchers reported a 100% disease control rate. All three patients with NSCLC achieved confirmed responses. The results support preclinical data that showed “synergistic activity” of joint PRMT5/RAS inhibition, Peters said. Brian M. Wolpin, MD, MPH, who presented the RASolute 302 findings during ASCO’s plenary session, said the phase 1/phase 2 data of the vopimetostat-daraxonrasib combination build on “the monotherapy activity” the investigational agents previously showed. “Pancreatic cancer remains a largely intractable disease and an area where patients desperately need new therapies,” Wolpin, director of Hale Family Center for Pancreatic Cancer Research at Dana-Farber Cancer Institute, said in the release. “In the front-line setting, chemotherapy has long been the standard of care, yet it presents significant tolerability challenges and overall limited efficacy against this aggressive disease. … These early combination data demonstrated the potential to meaningfully reshape how we treat this disease with a precision-guided, chemotherapy-free approach.” The Tango Therapeutics press release described the vopimetostat-daraxonrasib combination as “generally well tolerated” across dose levels, with most adverse events being grade 1 or grade 2. The most common treatment-related adverse events included rash, stomatitis/mucositis and diarrhea. Two patients assigned the higher vopimetostat dose experienced dose-limiting toxicities. One developed grade 3 rash. The other developed grade 3 stomatitis and fatigue. No patients discontinued the combination due to adverse events, and no treatment-related grade 4 or grade 5 adverse events occurred. Published by: Ask a clinical question and tap into Healio AI’s knowledge base. PubMed, enrolling/recruiting trials, guidelines Clinical Guidance, Healio CME, FDA news Healio’s exclusive daily news coverage of clinical data Learn more Add topic to email alerts Receive an email when new articles are posted on Please provide your email address to receive an email when new articles are posted on . “ data-action=”subscribe”> Subscribe We were unable to process your request. Please try again later. If you continue to have this issue please contact customerservice@slackinc.com. Back to Healio Source link

Facts About Social Anxiety – HealthyWomen
May is Mental Health Awareness Month. Pleasantries were the stuff of nightmares for Kristen Rogers. A random run-in with a coworker would cause her heart to pound so hard she thought it would leap out of her chest. Her mind would go blank — she’d stammer trying to make conversation while pools of sweat collected under her arms. Even impromptu chats with close friends or family caused this type of extreme anxiety. But the fallout was even worse. “I would always end those interactions feeling really embarrassed and ashamed, and I’d ruminate for hours or days about how the other person must think I’m stupid or incompetent,” Rogers said. “I would get so upset and stressed and physically sick — it was an unfortunate cycle.” Rogers was a teenager when the symptoms started and they only intensified as she got older. She didn’t date or make a lot of new friends — she wouldn’t even dance at concerts because she was terrified that everyone was watching her. Judging her. Rogers figured she was just an anxious person. But when she started seeing a psychiatrist in 2020, she learned it wasn’t just anxiety — she had social anxiety disorder. What is social anxiety disorder? Social anxiety disorder (SAD) is the persistent, intense fear of social or performance situations where a person anticipates being scrutinized, judged or humiliated. For people living with SAD, common everyday activities like talking to new people, eating in public or giving a presentation at work can cause crippling anxiety and fear. “When you have social anxiety disorder, that fear of being revealed as inadequate or worrying that people are going to judge you gets in the way of life,” said Ellen Hendriksen, Ph.D., psychologist and author of How to Be Yourself: Quiet Your Inner Critic and Rise Above Social Anxiety. Hendriksen said people with social anxiety experience distress, impairment or both. Distress in this context means discomfort, stress, anxiety and feeling upset before, during and/or after a social interaction. Impairment meaning social anxiety stops you from doing things you want to do. “If you turn down a promotion at work because it would make you have to go visit satellite offices and talk with a lot of strangers — that’s impairment,” Hendriksen said. People living with SAD also experience physical reactions such as blushing, rapid heart rate, nausea, trembling, lightheadedness and difficulty talking in social situations. “You might feel your stomach drop, you might turn red, you might get sweaty — all the classic fight or flight physical symptoms,” Hendriksen said. Symptoms of SAD can vary from person to person and change over time. And while it’s completely normal to feel nervous or anxious now and then, SAD is a chronic medical condition that requires treatment. The root of social anxiety Social anxiety disorder isn’t caused by one thing. Instead, SAD is usually a combination of biology, life experiences and learned patterns, according to Laura Johnson, LMFT, LPCC, cognitive behavior therapist and author of Social Anxiety For Dummies. When it comes to biology, Johnson said people with SAD may be born with a tendency to be inhibited. “Social anxiety could be linked to having an overactive amygdala, the part of the brain that controls your fear response.” Having a family history of SAD may also increase risk. One study found people with a first-degree relative (parents, sibling) with SAD are up to six times more likely to have the disorder. And because SAD usually starts in childhood or early teenage years, negative life events such as abuse, neglect or growing up with a medical condition that causes unwanted attention and how your parents raised you can be risk factors for SAD. “Some ways your parents could have influenced the development of social anxiety include modeling anxious behaviors, being overly protective or being critical,” Johnson said. Women and social anxiety disorder SAD affects both men and women, but research shows women are more likely to have SAD — and have more severe symptoms as well as higher levels and greater numbers of social fears — compared to men. “From a young age, many women are subtly — and sometimes not so subtly — taught to be agreeable, likable and not take up too much space. That can translate into over-monitoring how they come across, second-guessing their own opinions and holding back in conversations, especially in environments like the workplace where men may dominate discussions or interrupt, which can further reinforce self-doubt,” Johnson said. Although SAD typically develops earlier in life, major life events such as moving to a new city or being diagnosed with an illness may trigger symptoms in adulthood for the first time. “Women in midlife with social anxiety disorder have probably had it for decades and the key thing to know is that social anxiety disorder is fed and watered and maintained by avoidance, so it’s important to try to face your fears and think about where you’ve built avoidance into your life,” Hendriksen said. Social anxiety never goes away — but it can get better The most common treatments for social anxiety disorder are prescription medications and cognitive behavioral therapy (CBT), which involves identifying and reframing negative or irrational thoughts over time. “The most effective treatment is cognitive behavior therapy, especially when it includes exposure,” Johnson said. “That means gradually facing the situations you fear instead of avoiding them, while also learning how to respond differently to the thoughts driving the anxiety.” Exposure exercises involve identifying the fear and worst-case scenarios in social situations and testing them out to see if the outcome is really as bad as the person with SAD thinks it would be. “The point is to face our fears, and our feared outcomes are almost always worse than what actually happens. Even if the worst-case scenario happens, we have to remind ourselves that we are able to cope and that we can handle what life throws our way,” Hendriksen said. For Rogers, CBT made a huge difference. “In a

9 G-Spot Sex Positions That Might Just Blow Your Mind
In recent years, the G-spot has been the subject of more headlines than Taylor Frank Paul or Taylor Swift combined. For good reason: This long-misunderstood, once-controversial erogenous zone can facilitate some freaking pleasurable play. If you’ve still got questions, fear not. We’re breaking down everything you need to know about G-spot stimulation, including expert tips and the best G-spot sex positions to try tonight. What (and where) is the G-spot? Short for the Grafenberg spot, the G-spot is that magical area located about two inches inside the vaginal opening on the anterior (front) upper wall, closest to your tummy, explains Gigi Engle, a COSRT-certified sex and relationship psychotherapist, author of Kink Curious. When you’re aroused, this ball of tissue swells and can become highly sensitive when stimulated. Whether via body part or toy, when stimulated through penetrative play, it can create a tingling effect and/or a feeling of fullness that some pleasure-seekers enjoy, she says. Related story From Friction Burns to Falls, Sex Injuries Are More Common Than You Think It’s important to note that the G-spot is less of a button and more like “the whole zone of the top of the vaginal wall,” says Tara Suwinyattichaiporn (aka Dr. Tara), PhD, a sex and relationship coach, sex expert on TikTok, and professor of relational and sexual communication at California State University Fullerton. It’s best understood as part of a larger internal pleasure network that includes the internal structures of the surrounding erectile tissue, the urethral sponge, and the Skene’s Glands, Engle tells SheKnows. How to stimulate your G-spot during sex The G-spot is relatively shallow (aka not deep in the vagina), and generally responds best to consistent pressure, per Engle. So, the secret sauce for stimulating the G-spot—and maybe even facilitating a full-blown G-spot orgasm—is to marry shallow penetration with pressure. Sex toys with a curved shape and bulbous tip do well to stimulate this erogenous zone, as their unique shape makes it easy to maintain contact with the front vaginal wall, says licensed clinical social worker and AASECT-certified sex therapist Shamyra Howard, PhD, CST, LCSW. Vibrating G-spot toys will transmit vibrations deep into this erogenous zone and deeper clitoral network, she says. Meanwhile, options made from heavier materials like stainless steel or glass can also increase that pressure, since they naturally exert more weight than lighter silicone toys. While the G-spot often responds well to firmer stimulation, “for the best experience, this area should be approached slowly, gently, and gradually increasing in intensity,” sex coach Jenna Switzer tells SheKnows. It isn’t until you’re already aroused that the G-spot fills with blood, which makes it both easier to find and more sensitive, she explains. Going from zero to pressure can feel uncomfortable at best and painful at worst. That said, even with proper warm-up you may not go goo-goo ga-ga over having your G-spot stimulated. “This area has a ‘hit or miss’ vibe to it,” says Switzer. While some people “may experience an increase in lubrication, intense orgasms, and/or ejaculation (aka squirting),” others find stimulating this area uncomfortable or unpleasant. Others still don’t feel much different at all. “Some people experience it as erogenous and some do not — just like some of us enjoy having our feet rubbed and others find foot rubs annoying,” Jess O’Reilly (aka Dr. Jess), PhD, Astroglide’s resident sexologist, tells SheKnows. The Best G-Spot Sex Positions Ready to explore your G-spot? These expert-approved sex positions are designed to give you the best angle, depth, and control for maximum pleasure—whether you’re hoping to squirt, intensify your orgasms, or just mix things up. Not every position will work for everyone, but they’re a great place to start for beginners looking to explore this sensitive area or seasoned veterans ready to shake things up. And of course, as with all sex and sexual positions, be sure to give your partner plenty of feedback and modify the positions as needed. A version of this story was published in October 2018. Lifted Missionary Image Credit: Sasha Purdy/SheKnows That’s right, this classic can moonlight as a G-spot sex position with one simple tweak. Just like traditional missionary, the receiving partner lies on their back while the penetrating one lies over them. The difference? The bottom partner places a pillow or wedge under their butt, which lifts the hips and changes the angle of the vaginal canal. Why it’s great: Placing a pillow under the receiving partner’s hips “tilts the pelvis so that the penetrating part is naturally angled toward the front vaginal wall,” explains Engle. The result: Anything that enters the body is much more likely to rub directly against the G-zone, she explains. Coital Alignment Technique (CAT) Image Credit: Sasha Purdy/SheKnows Its name might be a mouthful, but if shallow, sustained stimulation is your thing, you will love this G-spot sex position. Coital Alignment Technique (CAT) requires the same set up as missionary: The receiving partner lies on their back, while the penetrating partner gets on top. The difference lies in how the top partner moves once inside. “Rather than thrusting in and out, the penetrating partner shifts their body slightly higher so their pelvis rests against the bottom partner’s vulva,” explains Engle. From there, the top partner rocks side to side while keeping their bodies closely connected. Why it’s great: “This technique keeps pressure directed toward the G-spot area and the internal clitoral structures more broadly,” explains Engle. Unlike fast, jack-rabbit-esque thrusting, this steady contact can feel more pleasurable for people who prefer pressure over intensity or depth. Rider on Top Image Credit: Ashley Britton/SheKnows. Save a horse, ride a cowboy with G-spot position, which puts the person with the G-spot on top. Start with the penetrating partner leaning at a 45-degree angle against a wall, couch back or headboard. Next, the other partner saddles up, straddles them, and lowers down. Why it’s great: “Sitting on top of a partner may be the best way to stimulate your G-Spot, as you can control the angle of penetration,”
Bepirovirsen achieved functional cure in chronic HBV
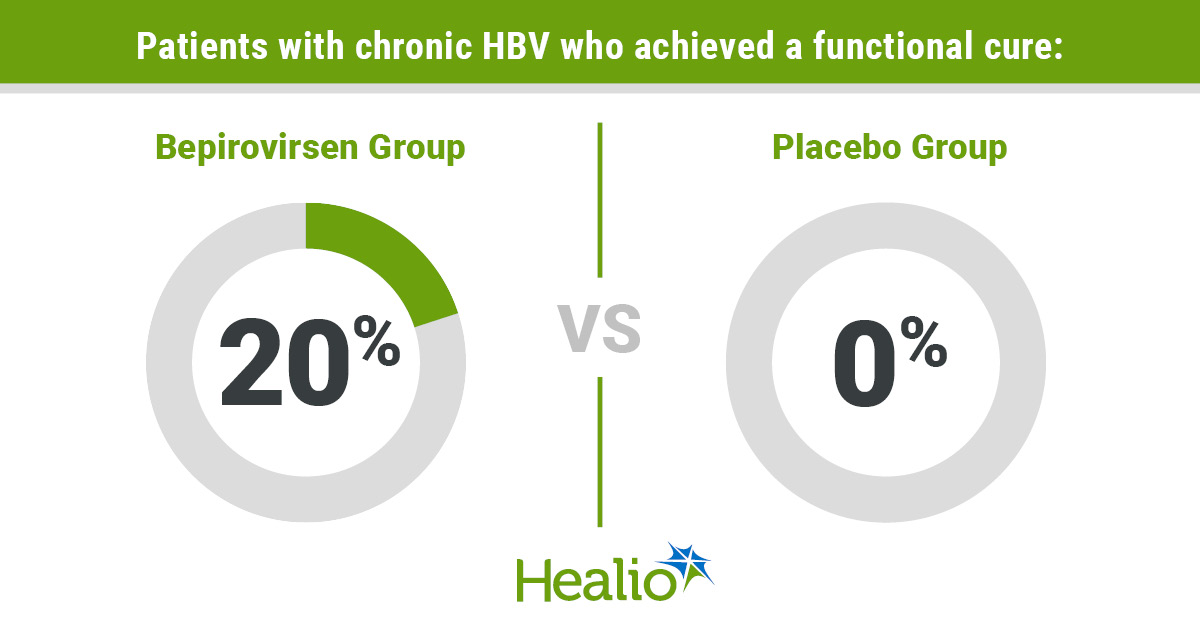
The B-Well 1 and B-Well 2 studies found that among individuals with baseline HbsAg less than or equal to 3,000 IU/mL, 20% and 19% achieved functional cure, respectively, as did 25% and 28% of those with baseline HBsAg less than or equal to 1,000 IU/mL. This is the first phase 3 study to date to achieve functional cure in a significant proportion of study participants. Although the phase 2b B-Clear study had previously shown that 9% to 10% of patients treated with bepirovirsen achieved functional cure in a smaller cohort, it identified a cut point of 3,000 IU/mL of HBsAg, under which up to 25% of patients were able to achieve functional cure. This led to the development of the phase 3 program, in which only patients with HbsAg less than or equal to 3,000 IU/mL were included. These phase 3 results confirm that functional cure can be achieved in these individuals, but that rates are highest among those with baseline HBsAg less than or equal to 1,000 IU per mL. Notably, although bepirovirsen was well-tolerated overall, 24% of treated patients experienced flares in their ALT level of at least three times the upper limit of normal during treatment, although many of these flares were associated with declines in HbsAg. There were other adverse events reported, including injection-site reactions, renal dysfunction and hematologic abnormalities, which were monitored closely during the trial. Most of these events were not severe. As such, results will hopefully contribute to potential approval of bepirovirsen for treatment of chronic HBV and a functional cure in select individuals, study authors said. There are a few limitations to the study worth noting. The population included was predominantly Asian and male, and results may not be fully extrapolated to patient populations from other demographic backgrounds or genotypes of HBV infection. Most patients were HbeAg negative, and therefore HbeAg-positive patients were not as well studied, although this reflects the patient population most seen in clinical practice. No patients were included that had HbsAg titers greater than 3,000 IU/mL, and it will be unlikely that patients with higher HbsAg levels would benefit from this treatment. Nonetheless, the results of this study are potentially practice changing and — for the first time in HBV drug development history — can potentially lead to a functional cure among many individuals living with chronic HBV. Further research should evaluate predictors of response among those individuals with HBsAg less than 1,000 IU/mL and less than 3,000 IU/mL, as well as data on potential stopping rules for treatment of individuals who do not respond to treatment. Additionally, it will be important to understand the degree of monitoring that will be required for individuals who initiate treatment with this regimen, if approved for use in clinical practice. All of this being said, these data are a historic moment in HBV history. For the first time, we can begin to tell our patients that functional cure is finally attainable. Reference: Yuen M, et al. N Engl J Med. 2022;doi:10.1056/NEJMoa2210027. Tatyana Kushner, MD, MSCE Weill Cornell Medicine Disclosures: Kushner reports advisory roles with or research support from Gilead Sciences, GSK, Ipsen, Madrigal Pharmaceuticals, Mirum Pharmaceuticals and Vir Biotechnology. Source link

5 Surprising Things that Can Affect Blood Pressure
May is Hypertension Awareness Month. The usual suspects — obesity, genetics, stress, salt intake, tobacco and alcohol use — affect your blood pressure. But did you know there are some things you may not have thought about? For some people, it’s cold medication. We all know decongestants are great for opening up a stuffy nose, but they also make it harder for blood to flow, which can increase blood pressure. As it turns out your blood pressure can be affected by a lot of things. Ironically, even going to see your healthcare provider (HCP) for a blood pressure check can cause a rise in levels, also known as “white coat syndrome.” A spike in blood pressure here or there is usually nothing to worry about, but chronic high blood pressure can be deadly. This is especially important for women to note as nearly half of all women in the U.S. have high blood pressure, and less than 1 in 4 have it under control. What is high blood pressure, and how serious is it? High blood pressure, also known as hypertension, is a serious chronic condition that affects 120 million people in the U.S. “That’s almost half the people in the country,” said Michelle Kelsey, M.D., a general cardiologist and associate professor at Duke’s School of Medicine. Hypertension causes the force of blood to push against your artery walls with pressure that is consistently too high. “This makes your heart work harder to pump blood and can lead to heart attacks, stroke or other serious health conditions over time,” Kelsey explained. “Hypertension is often called a ‘silent killer,’” Kelsey said.“While hypertension is asymptomatic in most people, you really have to check it to know.” Here are 5 surprising things that can increase your blood pressure: 1. Dehydration – Missing an occasional glass of water isn’t a big deal. But consistently running your body on empty can cause your blood pressure to drop, at first. “You feel light-headed and woozy, while your body tries to compensate by squeezing your blood vessels and hanging onto salt,” Kelsey explained. Over time, this can lead to high blood pressure. 2. Sleep apnea – Sleep apnea occurs when your breathing starts and stops at night while you sleep. This disrupts your ability to get restorative sleep and reduces your oxygen intake. Sleep apnea can be caused by living with overweight or obesity (which can be a risk factor for hypertension itself) or a structural issue that causes an obstruction in the airways as you breathe. “The drops in oxygen levels put stress on your body, which can lead to high blood pressure,” Kelsey said. 3. Chronic pain – Similar to the way stress can cause blood pressure to rise, chronic pain also triggers stress in the body and an adrenaline response that can cause full blown hypertension over time. One study found people with chronic widespread pain had a 75% increased risk of high blood pressure, while people with short-term pain had a 10% higher risk. 4. Loneliness – Social isolation and social stressors, like feelings of loneliness, can increase stress and contribute to the development of high blood pressure.One study of adults ages 45 to 85 found that the women who were single and had limited social activity had higher than average blood pressure. And if you have high blood pressure, not having someone to check in on you or take you to appointments can worsen the problem, according to Kelsey. 5. Nonsteroidal anti-inflammatory drugs (NSAIDs) – Popping an ibuprofen (Advil), naproxen (Aleve) every day may seem innocent enough, but it may also raise your blood pressure. NSAIDs inhibit cyclooxygenase (COX) enzymes, which leads to sodium and water retention in the kidneys, reduced blood flow and narrowed blood vessels. Talk to your healthcare provider It’s important to keep track of your blood pressure. The risk for hypertension increases with age so you could be walking around with high levels that increase your risk for heart attack and stroke and not even know it. Your healthcare provider can assess your risk and check your blood pressure regularly to see if medications or lifestyle changes are needed. “Knowing your numbers can be empowering,” Kelsey said. Source link
OrganTech Aims to Regenerate Hair and Teeth
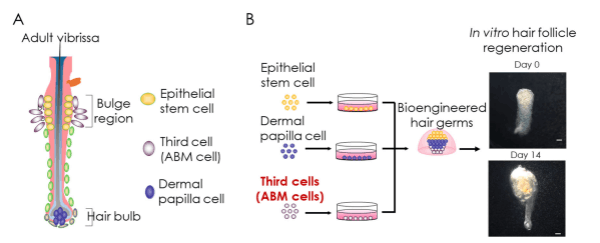
I have covered Japan-based OrganTech (previously known as Organ Technologies) for many years due to the company’s affiliation with founder Dr. Takashi Tsuji and RIKEN (Japan). I have covered Dr. Tsuji’s groundbreaking hair loss cure related work for over 12 years. This post was first written in 2020, and I regularly update it with the latest developments on top. Update: June 4, 2026 Injecting the “Third Cell” Planned for 2027 A day after I made the below major update yesterday, Dr. Tsuji granted a new interview to a Japanese website (h/t “Theo”) with some very interesting points. A therapy involving injecting “the third cell” into the affected area of hair loss is planned for 2027. Following that, the goal is to transplant hair follicle seed cells containing the third type of cell by 2028. Finally, the transplanting of regenerated hair follicles cultured in vitro (third generation) will occur by the 2030s. I am not sure from the translation whether the 2027 first generation treatment will be available to all (or just for clinical trial participants). The estimated cost (for the third generation treatment I think) will be around 20 million Japanese yen (equivalent to $125,000). This matches the lower end of the 20 million to 40 million yen estimate that Dr. Tsuji announced in 2019, albeit before the new “third cell” discovery. They plan to reduce costs to around 5 to 10 million yen down the road. I assume that the first generation 2027 treatment will be a lot cheaper. Key quote from Dr Tsuji: “The crucial difference with the third generation is that they are cultured outside the body, and seedlings are grown from seeds and then transplanted. Just like with rice cultivation, it is more reliable to plant seedlings that have properly developed than to sow the seeds and pick what grows.” Update: June 3, 2026 OrganTech gets Financing and Dr. Tsuji gets the Attention of the BBC In a great development, OrganTech just announced the successful completion of a financing round to support its next stage of growth. Some of these new funds will go into “accelerating the hair regeneration research and business development” related to the “Third Cell Type”. I discussed these “Third Cell” findings in my prior two updates from earlier this year. Long-time readers of this blog may remember how the first iteration of OrganTech (Organ Technologies) had to fold due to lack of funding. In 2021, I even tried to help RIKEN raise funds per their request (since I had so much respect for Dr. Tsuji). Also of significance, Dr. Tsuji got major coverage today in an article about women’s hair loss in the BBC. In the past, he almost never got any mentions in western media. Interestingly, they skipped covering almost all of Dr. Tsuji’s past two decades of work. The focus is just on the 2026 “novel third cell type” breakthrough finding, which Dr. Tsuji describes as a potential game changer in the treatment of alopecia. Update: May 20, 2026 Production of Hair Regeneration Supporting “Third Cell” Begins OrganTech has granted a manufacturing license to Kojin Bio (Japan) for the production of the “Third Cell” (hair follicle regeneration support cell). The latter was discussed in my last update. Apparently, Kojin Bio already sells a high-performance culture medium that enables the cultivation of dermal papilla cells and hair follicle regeneration supporting cells. Note that the artificially created “third cell” assists adult hair follicle-derived epithelial stem cells and dermal papilla cells to progress beyond hair bulb formation to actual hair shaft production. Update: February 21, 2026 OrganTech and RIKEN Scientists Discover “Third Cell” that Produces Hair OrganTech “third cell” for hair regeneration. Assists adult hair follicle–derived epithelial stem cells and dermal papilla cells to progress beyond hair bulb formation to sustained down-growth and hair shaft production. OrganTech and RIKEN just published a new study regarding the identification and subsequent artificial creation of a “third cell” to induce hair growth in mice. They first made the discovery of a previously unrecognized accessory mesenchymal cell population that is indispensable for functional hair follicle regeneration. When this new third cell was added to two existing cells (that had previously been identified as necessary for hair production), they were able to create a hair-producing organ. If applied to humans, this could lead to the development of new treatments for alopecia. The plan to begin clinical trials by the end of 2026. More details can be found on their website. “Specifically, the investigators describe a “third cell type,” termed hair follicle regeneration–supporting cells, which enables adult hair follicle–derived epithelial stem cells and dermal papilla cells to progress beyond hair bulb formation to sustained downgrowth and hair shaft production.” Edit: This news is now being published in many different publications. The latest eye catching headline: “Scientists Built Working Hair Follicles in a Lab. They Could Cure Baldness Forever.” It was already known that epithelial stem cells and dermal papilla cells are important for hair follicle regeneration. But while the presence of a ‘third cell’ was considered essential for hair follicles to enter the growth phase and produce hair, its identity remained unknown for a long time per Dr. Tsuji. In contrast to the conventional hypothesis that it was fibroblasts or adipocytes, the Tsuji team discovered a new group of cells in the mesenchymal region surrounding the bulge region of the hair follicle. These hair follicle regeneration supporting cells lead to the down-growth phenomenon in which hair follicles extend into the deeper layers of the skin. “The discovery that a third type of cell divides and powerfully pushes the tip of the hair follicle deeper into the skin is a groundbreaking achievement that overturns previous research. Mouse experiments have demonstrated that fully functional hair follicles can be regenerated by stacking these three types of cells vertically.” Update: July 12, 2025 HairDao’s much anticipated interview with Dr. Tsuji is out. I am traveling outside the country right now and won’t get a chance to listen to it till tomorrow. Update:

Medical accreditors commit to HHS nutrition education reforms
Add topic to email alerts Receive an email when new articles are posted on Please provide your email address to receive an email when new articles are posted on . “ data-action=”subscribe”> Subscribe We were unable to process your request. Please try again later. If you continue to have this issue please contact customerservice@slackinc.com. Back to Healio Key takeaways: Medical accreditors, assessors and organizations have joined HHS’ nutrition education initiative. Also, 19 more medical schools pledged to implement 40 hours of nutrition education or a competency equivalent. HHS and the U.S. Department of Education announced several developments in their efforts to improve nutrition education in medical schools. According to an HHS press release, eight medical accrediting, assessment and board organizations have “committed to implementing reforms aimed at instilling measurable nutritional education across key medical training programs.” The groups are: Eight medical accreditors, assessors and organizations and 19 more schools have joined HHS’ nutrition education initiative. Image: Adobe Stock the National Board of Medical Examiners; the Accreditation Council for Continuing Medical Education; the Accreditation Council for Graduate Medical Education; the Liaison Committee on Medical Education; the National Board of Osteopathic Medical Examiners; the Commission on Osteopathic College Accreditation; the American Association of Colleges of Osteopathic Medicine; and the American Board of Medical Specialties. HHS also announced that 19 additional medical schools have voluntarily committed to requiring at least 40 hours of nutrition education or a competency equivalent beginning this fall. They join the 54 other medical schools that previously pledged to these voluntary commitments when HHS first announced the initiative in March. “We’re putting nutrition education at the forefront of medicine and prevention at the forefront of health care,” HHS Secretary Robert F. Kennedy Jr. said during a press briefing. “We’re training future physicians to address the root causes of diseases, not simply manage their consequences. And we’re building a medical system that gives doctors better tools, patients better information, and families a better chance to live long, healthy lives.” HHS’ efforts to improve nutrition education under the second Trump administration began last year when the agency urged medical schools to immediately implement nutrition requirements into learning, such as continuing education, board certification and pre-medical standards. In a 2022 survey, medical students reported receiving just 1.2 hours of formal nutrition education yearly, the release said. Before these recent commitments, three-fourths of U.S. medical schools did not require nutrition courses and just 14% of residency programs mandated a nutrition curriculum. “While these commitments are groundbreaking, they are also rooted in common sense,” Under Secretary of Education Nicholas Kent said during the briefing. “From adding required nutrition hours to integrating competencies across all 4 years and revising assessments, these actions promise real progress toward our shared goal of a healthier America.” Jessica Snowden, MD, MS, MHPTT, vice chancellor for research at the University of Tennessee Health Science Center, said HHS’ initiative “recognizes something we all see every day in our clinical work and in our communities: nutrition is not a side issue in health care. It’s fundamental to many of the things we need to have a healthy lifespan.” “One of the things that is most exciting for me about this particular initiative is the opportunity to connect scientific evidence and nutrition education with real-world implementation,” she said. “As universities, we help generate the evidence that informs what’s going to move forward. We train the workforce. We evaluate outcomes to help you figure out what works and what doesn’t work. Importantly, we can help you figure out how to scale things so that they are implementable in a variety of communities.” Robert Glatter, MD, FACEP, FAAEM, an assistant professor at the Zucker School of Medicine at Hofstra/Northwell, told Healio that HHS’ call for greater nutrition education “represents an important opportunity to align physician training with the clinical realities of chronic disease prevention and management.” Robert Glatter “For physicians, the issue is not whether nutrition should replace pharmacologic or procedural therapies when indicated. It should not. The issue is whether clinicians can competently address one of the most powerful modifiable determinants of long-term outcomes,” he said. “Medical students should graduate being able to obtain a focused dietary history, recognize major dietary risk patterns, interpret nutrition labels, screen for food insecurity and deliver brief, evidence-based counseling that is culturally and economically realistic.” The goal, Glatter added, is to ensure that physicians can “integrate nutrition into prevention and chronic disease care.” “Strengthening nutrition education in medical school is therefore not curricular ornamentation; it is core clinical training,” he said. For more information: Robert Glatter, MD, FACEP, FAAEM, is an emergency medicine physician at Lenox Hill Hospital. He can be reached at rglatter@northwell.edu; Instagram rdglatter; LinkedIn https://www.linkedin.com/in/dr911/; and X @DrRobertGlatter. Sources/Disclosures Source: Press Briefing Reference: Disclosures: Healio could not determine relevant financial disclosures at the time of publication. Ask a clinical question and tap into Healio AI’s knowledge base. PubMed, enrolling/recruiting trials, guidelines Clinical Guidance, Healio CME, FDA news Healio’s exclusive daily news coverage of clinical data Learn more Add topic to email alerts Receive an email when new articles are posted on Please provide your email address to receive an email when new articles are posted on . “ data-action=”subscribe”> Subscribe We were unable to process your request. Please try again later. If you continue to have this issue please contact customerservice@slackinc.com. Back to Healio Source link

The Symptoms Were There, the Healthcare Providers Weren’t
June is National Cancer Survivors Month and Uterine Cancer Awareness Month. When heavy vaginal bleeding sent Julie Herbert to a California emergency room in November 2024, cancer was the furthest thing from her mind. A triage nurse at the hospital was very concerned, and the 36-year-old research associate was quickly admitted. “They immediately put me into a room and gave me IV fluids and a blood transfusion,” Herbert said. A Pap test administered by the hospital came back abnormal. After follow-up testing, including a CT scan, an ultrasound and a biopsy, Herbert was diagnosed with advanced cervical cancer that had spread to her lymph nodes. “When they told me it was cancer, I was stunned,” she said. After all, seven days earlier, she had seen a gynecologist for abnormal bleeding. Herbert said the doctor had attributed this to heavy menstrual periods and the recent removal of her intrauterine device (IUD), and did not order any follow-up testing. Herbert — who’d been using an IUD for eight years — had had the device removed three months earlier. She’d experienced some bleeding on and off before it was removed, but it got worse after it was taken out. Bleeding can occur when an IUD is removed, but excessive, prolonged bleeding after a removal may indicate a more serious underlying medical condition. Given her history of bleeding and the intensity of it, Herbert believes the medical professionals that she saw should have done more. “They said this could just be my body getting back to normal after getting the IUD out and blamed it on my hormones,” Herbert said. Herbert’s experience is not uncommon. Ignoring abnormal bleeding can have serious consequences Abnormal vaginal bleeding — or abnormal uterine bleeding (AUB) when it originates in the uterus — affects up to 35% of women and is defined as bleeding that is unexpected or prolonged, including extremely heavy periods or irregular bleeding not related to menstruation. But despite its prevalence, and the fact that abnormal bleeding is a common symptom of gynecologiccal cancers, it is frequently overlooked or attributed to fibroids, hormones, irregular periods, birth control or cervical polyps — potentially leading to a missed diagnosis of a more serious problem. “Cancer can happen to anyone, and my bleeding was not taken as seriously as it should have been,” Herbert said. Medical gaslighting compounds the problem Medical gaslighting — when medical providers invalidate or dismiss patients’ questions, symptoms or concerns — is a significant issue in women’s health, particularly in cancer care. This can happen with all patients, but marginalized communities are often particularly affected. A study published in BMC Women’s Health found that women have “consistently reported poor experiences in accessing care” for abnormal uterine bleeding throughout the last 20 years. Elena Ratner, M.D., a gynecologic oncologist at Yale Cancer Center, said that she frequently has patients come to her after they have seen numerous other medical providers who did not address their unexpected bleeding. “Abnormal bleeding is a tangible, clear symptom that should not be ignored, yet women are not being listened to,” Ratner said. Abnormal bleeding can happen for many different reasons and is not always a sign of cancer, Ratner explained. “However, it is essential that patients are properly evaluated to determine the cause, particularly since early diagnosis is crucial for gynecological cancers,” she added. Women’s pain has been normalized Several recent studies have found a gender pain bias, where medical providers assume women are exaggerating their pain. Menstrual pain and bleeding are also frequently seen as an inevitable experience for women, which leads to symptoms not being taken as seriously — even though tumors on the uterus and ovaries can cause pressure and pain that are similar to menstrual cramps. Ami Vaidya, M.D., an oncologist and co-chief of the Division of Gynecologic Oncology at Hackensack Meridian John Theurer Cancer Center, said that the ongoing normalization of menstrual-related pain and bleeding can cause patients to delay seeking help and may lead healthcare providers (HCPs) to overlook symptoms of a critical medical issue. “There is a significant and well-documented misconception in medicine where abnormal bleeding is sometimes dismissed as a normal part of ‘being a woman,’ which can lead to missed or delayed diagnoses of serious conditions,” said Vaidya. Despite diagnostic challenges, experts emphasize there are specific symptoms to gynecologic cancers that patients should be aware of and speak with their provider about, including: Abnormal bleeding — Any bleeding that is unexpected or prolonged, including extremely heavy periods or irregular bleeding not related to menstruation. Abnormal bleeding can be a symptom of each of the six types of gynecologic cancers — cervical, ovarian, uterine, vaginal, vulvar and fallopian tube (which is rare). Postmenopausal bleeding — If a patient is postmenopausal, meaning that they have not had a period in 12 months — any bleeding or spotting should not be ignored. Changes in menstruation — Heavier and/or longer menstrual bleeding than usual Urinary changes — Difficult, frequent or painful urination Pain or bleeding during or after intercourse — Any discomfort or spotting related to sexual activity Swelling or bloating — Feeling swollen or bloated in the lower abdomen Digestive changes — Changes in appetite, indigestion, nausea and chronic constipation Vaidya said there are different diagnostic exams that patients can discuss with their HCP that may help determine the cause of abnormal bleeding, including: Pelvic exam and Pap/HPV tests Blood tests to check for anemia or hormonal issues Transvaginal ultrasound to identify structural problems Endometrial biopsy to examine the uterine lining for cancerous cells Hysteroscopy for a direct visual inspection of the uterus Vaidya recommends that patients keep a symptom journal to track any pain and/or bleeding and bring a list of questions to their medical appointments. “If you feel dismissed, ask pointed questions such as, ‘What specific tests can we run to rule out more serious conditions like cancer?’ If a requested test is denied, insist that the doctor document the refusal in your chart — a step that often prompts action,”

Hers Is Making Popular GLP-1 Injections Affordable — Starting at $39
If you purchase an independently reviewed product or service through a link on our website, SheKnows may receive an affiliate commission. Turning to medications to help you reach your weight loss goals was once taboo, but with new advancements and telehealth platforms offering options such as Wegovy, Ozempic, and other treatments available online, it’s now a welcome tool for achieving weight loss. The only downside? These medications can cost a small fortune each month, and often require insurance. That’s why platforms like Hers offers a new model that makes GLP-1 injections and oral medication accessible, affordable, and straightforward. Not familiar with Hers? Hers is a telehealth program that provides personalized weight management plans and a comprehensive approach to weight loss, offering accessible medication options — including GLP-1 injections, oral weight loss medications, and compounded medications—at affordable prices. The platform combines prescription medications with in-app support from clinicians to help you achieve your health goals. Whether you’re looking for GLP-1 Injections, oral weight loss medications, or compounded medications, Hers makes it a breeze to obtain the medication best tailored to your needs. Ahead, learn more about Hers’ plans and medication pricing. Related story The Brand Famous for Designer Fashion Dupes Makes the Best Greens Powder—So You Can Stop Overpaying for Yours Learn more about Hers here. How the Program Works Hers’ weight loss programs operate on a subscription-based model, making medication costs affordable and accessible. Recently, the platform introduced a new membership model, which now features “a new, personalized approach to weight loss, combining FDA-approved medications with expert-led care and ongoing support, all delivered online,” per the brand. Now, customers can access Wegovy in two formulations: the FDA-approved oral Wegovy Pill or the injectable Wegovy Pen. These flexible options are available without insurance requirements. Before starting a prescription, you will complete an intake appointment — an initial online assessment that helps Hers understand your medical history and lifestyle. Available Medications Hers offers a variety of weight loss medications tailored to every budget and lifestyle. Below, see a quick list of its available options. GLP-1 Injections: Wegovy (semaglutide) and Zepbound (tirzepatide).Oral Medications: Bupropion, Metformin, Topiramate, Naltrexone, and Vitamin B12.Compounded Medications: More affordable, no-brand-name alternatives that offer lower costs. Cost Breakdown Hers’ new model includes a membership that helps keep costs transparent and affordable, with no surprises like those others experience on other weight loss platforms. Here’s how it works: – Hers users pay $39 for the first month, then $149/month thereafter– The Wegovy Pill starts as low as $149/month– The Wegovy Pen costs as low as $199/month The membership includes: – 24/7 access to messaging with licensed providers– A dedicated Care Team– Unlimited dosage adjustments– Personalized Weight Loss Care– Continuous provider access– Ongoing plan adjustments– Guidance across nutrition, movement, and sleep habits What the Reviewers Say Hundreds of Hers users report success with the platform. “Through my weight loss experience, I’m hoping to gain long-lasting results that I can maintain even after I get off the GLP-1,” one shared. “I chose Hers because it’s a brand that I’ve used in the past and it’s a trusted brand that I feel confident with.” “My family has a history of Type 2 diabetes,” another wrote. “While my doctor was in favor of prescribing Ozempic to me, it wasn’t covered by insurance. Thanks to Hers, I could access treatment. I am so happy with my results!” If you’ve been searching for an approach to achieving your weight loss goals without any success, head to Hers today. Its impressive reviews and affordable treatment plans make achieving your health goals even more accessible. About the Author Taylor Lane is a contributing commerce writer at SheKnows, covering beauty, style, and lifestyle. With over eight years of media experience, she previously served as a beauty writer at The Zoe Report and a fashion assistant at Glamour. Her work has appeared in StyleCaster, The FlowSpace, WWD, Forbes Vetted, Teen Vogue, InStyle, and more, where she’s tested hundreds of products — from top-performing mascaras to the most functional strollers. She’s also a mom of two girls, a ten-year-old and a 4-month-old. And when she’s not online, she’s usually at Pilates. Before you go, check out our slideshow below: Source link