

It didn’t take long at all for our bond to build once the adoption was confirmed. Even that first day of bringing him home in the car, I could feel he had established a sense of trust in me. From there, our connection continued to build, and we developed our daily routine: waking in the morning to take my medication followed by cuddles, getting out for our morning and afternoon walks (Bruce on timekeeping duties, of course!) and mealtimes right on schedule. As a result of having this routine, Bruce would also sense I was having my bad migraine days if I got up in the morning but wasn’t able to shower due to lack of balance, and he would be very patient, quiet, and forego his usual demands for outings, being quite happy to potter around in the back garden. If I needed assistance, I would shout “Bruce, here, help”, and he would come upstairs and stand by my bed, close enough for me to put my hand on his back so that I could stabilise myself to get up and stand. He then would walk beside me and somehow had learnt himself the best position to stand behind me when coming down the stairs, so that the weight of his body would support me behind my legs if I started to tip backwards or could put my hand there next to him to maintain balance. I didn’t teach him to do this; he just seemed to know what to do! When my migraine attack had lifted, and he would hear me go into the bathroom, the noise of the shower and see me come downstairs changed out of my pyjamas – that was it; action stations, and usual routine back on! Source link
#FGblog – Eosinophilic oesophagitis: the past, present, and future.
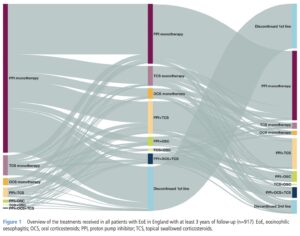
Eosinophilic oesophagitis (EoE) is an allergic disease of the oesophagus characterised by an elevated eosinophil count on oesophageal biopsy. It classically presents with dysphagia in adults; symptoms in children can be more varied, including abdominal pain and vomiting as well as dysphagia [1]. It is a relative newcomer in the world of gastrointestinal disease, first having been described just over 30 years ago, but its incidence is increasing, even taking into account increased knowledge of the condition and better diagnostic strategies [2]. In this #FGblog we want to draw Frontline Gastroenterology readers’ attention to two recent open access papers published in the journal on EoE; one offering insights into the real-world experience of EoE in England, and the other ways in which care for patients living with this condition can be improved. Xu et al. integrated and interrogated three national databases to evaluate EoE-related symptoms and comorbidities in 2381 patients with EoE compared to 9365 age and sex matched controls [3]. As might be expected, patients were predominantly male (70.1%) and young (median age 40). 29.2% of patients with EoE had one or more allergic comorbidity, the most common being asthma. Some of the more hard-hitting findings include the fact that 15.5% of patients had a diagnosis made 24-36 months after symptom onset. Factors associated with this prolonged time to diagnosis included having symptoms of acid reflux or heartburn, which would fit with symptoms being attributed to gastro-oesophageal reflux disease rather than EoE, but interestingly also with age less than 18 years old, and the presence of one or more EoE-related comorbidities. The latter finding is surprising, as the association of EoE with other allergic conditions has been known for a long time. 8.2% of patients presented with food bolus impaction, and 18.3% of patients developed strictures. Although this is the minority of patients, when the ground-level burden on patients and resource use is considered (e.g. emergency endoscopy, therapeutic dilatation), the impact of this ‘rare’ condition is huge. In terms of treatment, most received proton pump inhibitor (PPI) monotherapy as first line therapy, and if patients were switched, the most popular alternative was PPI with topical corticosteroid (TCS). Our second paper from Dhar et al. proposes an integrated care pathway to tackle some of the difficulties faced by patients living with and clinicians managing EoE [4]. The pathway agreed on in two expert group meetings are clear, evidence based, and will be for many, practice-changing. Out for good are non-recommended medical therapies for relieving food bolus obstruction such as buscopan, glucagon and Coca Cola (other ineffective fizzy drinks available). In are recommended time intervals to OGD of within 6 hours, 24 hours, or 2 weeks depending on whether the patient is distressed, stable but at risk of aspiration, or if the food bolus has passed respectively. More on recent advances in EoE can be found here [5]. The need for multiple oesophageal biopsies to increase diagnostic yield should be standard practice; the authors recommend at least six biopsies from multiple sites, ideally three. The diagnostic threshold recommended is >15 eosinophils per 0.3mm2 of oesophageal epithelium. First line medical therapy for induction of remission is unequivocally budesonide orodispersible tablet (ODT). PPIs and dietary interventions usually fail and result in more repeat endoscopies, and compliance with the strictest, more effective six-food elimination diet is low. Patients should also be on maintenance treatment once remission is achieved as relapse rates following treatment cessation are high. Once again, the best option is budesonide ODT, which is both effective and safe in achieving clinico-histological remission. We would strongly encourage readers to read the full versions of both of these excellent papers, which are certainly cause for reflection on the care we provide to people living with EoE. References Shillitoe B, Lee JC, Hussien M, et al. Clinical spectrum of paediatric and adult eosinophilic oesophagitis in the North East of England from 2016 to 2019. Frontline Gastroenterology 2022;13:231-236. https://fg.bmj.com/content/13/3/231 Dhar A, Haboubi H, Auth M, et al. Eosinophilic oesophagitis: improving diagnosis and therapy – reducing the burden of repeated endoscopy. Frontline Gastroenterology 2022;13:e51-e56. https://fg.bmj.com/content/13/e1/e51 Xu X, Chen SY, Maslova E, et al. Clinical symptoms, comorbidities, treatment patterns and time to diagnosis in patients with eosinophilic oesophagitis in England: a retrospective cohort study. Frontline Gastroenterology Published Online First: 08 August 2024. doi: 10.1136/flgastro-2024-102646 https://fg.bmj.com/content/early/2024/08/08/flgastro-2024-102646 Dhar A, Attwood S, Basu K, et al. Improving management of eosinophilic oesophagitis in adults in the UK: proposal for an integrated care pathway. Frontline Gastroenterology Published Online First: 12 August 2024. doi: 10.1136/flgastro-2024-102768. https://fg.bmj.com/content/early/2024/08/11/flgastro-2024-102768 Attwood S, Epstein J. Eosinophilic oesophagitis: recent advances and practical management. Frontline Gastroenterology 2021;12:644-649. https://fg.bmj.com/content/12/7/644 Author: Dr James Kennedy (Trainee Associate Editor) Twitter: @DrJMKennedy Declarations: I am a trainee associate editor for Frontline Gastroenterology (Visited 368 times, 1 visits today) Source link

Understanding Medications & Pharmacologic Options for Pain Management
Preventing Winter Falls: Balance and Strength Training Tailored for Cold Weather Challenges By Bob Berendsen • January 15, 2026 Winter, widely considered the season of comfort, is the time for indoor relaxation and quiet contemplation. However, winter also brings with it some very real dangers, including cold, dark, and slippery surfaces. For older adults or those dealing with chronic pain, a small slip on these surfaces can lead to serious injuries that take months to heal. The good news? You can train your body to handle these challenges. Let’s explore some simple, safe exercises you or your loved ones can do from the comfort of your home to build your winter-proof stability. Why Winter Increases the Risk of Falls Cold weather brings more than just chilly air. It changes the way we move, how our muscles respond, and even how we think about walking. When it’s icy, people tend to tense up, take shorter steps, and look down more often. Muscles also get tighter in the cold, which reduces flexibility. Plus, all those bulky layers of clothes mess with your center of gravity and limit how quickly you can react if you start to lose your balance. Your boots might be waterproof and warm, but they’re probably not giving you the ankle support or ground feel you’d get from your regular shoes. Then there’s the simple fact that many of us move less in winter. Maybe you skip your daily walks when it’s freezing, or you stop going to that exercise class because driving feels too risky. But here’s the catch: the less you move, the weaker you get, and the weaker you get, the more likely you are to fall. Building a Foundation To prevent this, you simply need to work on two main things: balance and strength. Physical therapy and balance-focused exercises train your muscles, joints, and nervous system to respond faster and more effectively when something throws you off. Balance Training Balance isn’t just about standing still without wobbling. It’s about how your body reacts when something throws it off center. When you step on ice, for example, your brain and muscles have to communicate in an instant to keep you upright. If that connection is slow or weak, you’re more likely to fall. Some simple ways to train your balance include: ● Single Leg Stands : Stand near a sturdy surface like a countertop or wall for support. Lift one foot slightly off the ground and hold that position for 10–15 seconds. Then switch sides. At first, you might wobble, but that’s perfectly normal. Over time, your legs, ankles, and core muscles will get stronger, and your balance will improve. Try doing 3 rounds on each leg daily. ● Heel-to-Toe Walk: Imagine you’re walking on a tightrope. Place one foot directly in front of the other, heel touching toe, as you move slowly across the room. This simple drill strengthens your stabilizing muscles and sharpens coordination. Keep your eyes forward, not down, and use a wall for light support if needed. ● Side Leg Raises: Hold onto a sturdy chair or counter. Lift one leg out to the side while keeping your back straight and your toes facing forward. Lower it slowly and repeat. This exercise builds hip strength, which plays a big role in staying upright on slippery ground. ● Weight Shifts: Stand with your feet hip-width apart and shift your weight from one leg to the other slowly. Feel your balance change from left to right. This gentle exercise teaches your body to adjust quickly. Strength Training Balance and strength go hand in hand. When your muscles are strong, they act like shock absorbers, keeping you stable even when your footing isn’t perfect. Focus on the muscles that support your posture and help you move safely. Here are a few simple exercises to include in your daily routine: ● Chair Squats: Sit down and stand up from a sturdy chair without using your hands for support. Keep your feet flat on the floor and your knees aligned with your toes. This move strengthens your thighs, hips, and glutes—key muscles for stability and control. ● Heel Raises: Stand behind a chair or counter and slowly lift your heels so you’re standing on your toes. Lower back down after holding for a few seconds. This helps strengthen your calves and ankles, improving the small muscle reactions that keep you upright when you slip. ● March in Place: Lift your knees high as if you’re marching. Do this for one to two minutes, rest, and repeat. Marching builds leg endurance and helps train your coordination. ● Core Squeezes: While sitting or standing, tighten your stomach muscles as if you’re zipping up a snug jacket. Hold for 10 seconds, then release. A strong core helps your upper and lower body work together to keep you balanced. These movements may look simple, but they’re powerful. Doing them for just 10–15 minutes a day can make winter walks safer and less stressful. Warming Up Before You Head Outdoors Cold weather tightens muscles and slows blood flow, making your body less responsive. That’s why warming up before heading outside is so important. Think of it as insurance against sudden slips. Try a short warm-up routine before stepping out: ● Arm circles to loosen shoulders. ● Gentle knee bends to wake up leg muscles. ● Shoulder rolls and neck stretches to improve mobility. ● A quick indoor walk or stair climb to raise your heart rate slightly. It’s also wise to check your footwear. Look for rubber soles with deep treads for better traction. Avoid smooth or worn-out shoes, and consider ice grips that attach to your boots if you live in a particularly snowy area. Winter doesn’t have to be a season of fear. By investing just 10-15 minutes a day in these simple, safe exercises, you can build the strength and confidence you need to navigate the season safely. You are giving your body the tools it needs to

What Is PMDD? – HealthyWomen
May is Mental Health Awareness Month and National Women’s Health Month. Mood swings. Bloating. Breast tenderness. The terrible trilogy can only mean one thing: Winter — sorry, your period — is coming. About 3 out of 4 people who menstruate experience symptoms of premenstrual syndrome (PMS) up to two weeks before their period actually starts. (Sidenote: If the math is mathing, that means women have around seven days a month that are PMS or Aunt Flo free. Just a reminder that women are amazing.) PMS is common, but for some women, the emotional and physical symptoms are so extreme they seriously impact the ability to function. This severe version of PMS is actually a mood disorder called premenstrual dysphoric disorder (PMDD). Read: 7 PMS Tips from the Pros >> What is PMDD? Premenstrual dysphoric disorder is a chronic condition that causes intense emotional and physical symptoms that start one to two weeks before your period and end a few days into your cycle. PMDD symptoms The physical and emotional symptoms of PMDD are extreme — so severe that they affect the ability to function at home, work and in personal relationships. PMDD symptoms can include: Feelings of sadness, hopelessness or worthlessness Anxiety Mood swings Self-critical thoughts and/or increased sensitivity Increased irritability or anger Increased conflicts with family, coworkers or friends Loss of interest in everyday activities Problems concentrating Fatigue Changes in eating patterns (binging, overeating or craving certain foods) Problems sleeping or sleeping too much Feeling overwhelmed or out of control Breast tenderness Headache Muscle aches Weight gain Bloating What causes PMDD? Research is ongoing as to what causes PMDD, but it may have something to do with the drop in hormone levels that happen after ovulation. Serotonin — a natural brain chemical that regulates mood — may also play a role. Serotonin levels fluctuate throughout the menstrual cycle and some people may be more sensitive to the changes. PMDD vs. PMS PMDD is like PMS on steroids. Here’s the difference: PMS symptoms are typically mild to moderate and don’t usually stop you from doing everyday activities. PMDD causes intense mental and physical changes that impact your everyday life and the way you interact with others. PMDD is a medical condition that should be diagnosed and treated by a healthcare provider. Risk factors for PMDD PMDD affects about 5 out of 100 people who menstruate. You may be at risk for PMDD if you: Have a family history of PMS or PMDD Have a personal or family history of mood disorders, depression or postpartum depression How do you get a diagnosis of PMDD? PMDD is defined by having five or more symptoms, including one that’s mood-related. In addition to going over your health history and a physical exam, a healthcare provider (HCP) will usually ask you to track your symptoms in a journal or diary for a period of time before making a diagnosis. PMDD treatments There are several medications and lifestyle changes that can help manage the wide range of symptoms associated with PMDD. PMDD treatments can include: Selective serotonin reuptake inhibitors (SSRIs) Over-the-counter (OTC) pain relievers Stress management and relaxation techniques Cutting down on sugar, salt, caffeine and alcohol may also help decrease some symptoms of PMDD. Read: Why Hormonal Birth Control Is So Important to Women’s Healthcare >> PMDD is a chronic condition For many people with PMDD, symptoms get worse over time and last until menopause. So, it’s important to talk to your HCP if you think you may have PMDD. There are treatment options that can help. From Your Site Articles Related Articles Around the Web Source link

The Hidden Health Risks of High Heels: From Posture to Pelvic Floor
With 26 bones, 33 joints, over 100 muscles, tendons, and ligaments, and thousands of nerve endings, the human foot is undeniably one of the most complex structures in our body. It is also one of the most vital: our feet support our entire weight, keep us upright, and act as shock absorbers for every step we take. Yet, instead of protecting them, many women subject their feet to “impossible” shoes. Driven by societal pressures to meet an aesthetic ideal, we often sacrifice our health for fashion. The price? Potentially irreversible damage to our feet, musculoskeletal structure, and circulatory system. The statistics are telling: 80% of patients with foot problems are women, and 90% of these issues stem from the habitual use of stilettos, narrow-toed shoes, or non-breathable synthetic materials. Common Foot Injuries Caused by Improper Footwear 1. Calluses These are thickenings of the skin formed by dead cell accumulation due to constant pressure and friction. While often dismissed as a cosmetic issue, they can cause pain, fissures, and infections, eventually altering your gait and posture. 2. Bunions (Hallux Valgus) A bony deformity at the base of the big toe. Symptoms include inflammation and chronic pain. If left untreated, bunions can lead to secondary issues like bursitis, hammertoes, or metatarsalgia. 3. Bursitis This is the inflammation of the bursa—small fluid-filled sacs that cushion the joints. It results in swelling, stiffness, and sharp pain in the toes and feet. 4. Hammertoes and Claw Toes This deformity causes the toe joints to bend abnormally. Over time, this curvature becomes permanent, making walking difficult and painful. 5. Metatarsalgia Intense pain in the ball of the foot (the metatarsus). This area is crucial for impact absorption and weight distribution; when it fails, postural stability is compromised. 6. Morton’s Neuroma A thickening of the tissue around the digital nerve (usually between the third and fourth toes), causing a sensation of “walking on a marble,” sharp pain, or numbness. The Domino Effect: Postural and Muscular Alterations When standing barefoot, the ball of the foot supports about 43% of your weight, while the heel takes 57%. High heels flip this ratio dangerously. The physical consequences include: Shortened Calves: The Achilles tendon loses flexibility and the calf muscles contract. Joint Overload: Excess pressure shifts to the ankles and knees. Pelvic Tilt: To compensate for the forward lean, the quadriceps and hips are forced into an unnatural position. The Impact on the Core and Pelvic Floor Perhaps the most surprising consequence is the link between high heels and pelvic floor dysfunction. Constant heel use weakens the “core” and can lead to: Urinary incontinence Organ prolapse (bladder or uterus) Sexual dysfunction (such as anorgasmia) Circulatory Problems: Beyond the Surface Improper footwear disrupts the “muscle pump” of the legs, making it harder for blood to return to the heart. This leads to Venous Insufficiency, which affects women five times more often than men. Chronic Venous Disease: Symptoms include varicose veins, edema (swelling), and a heavy sensation in the legs. Phlebitis: Inflammation of a vein that can escalate into Thrombosis, a blood clot that increases the risk of heart attack or stroke. How to Choose the Right Shoes: The 4 Golden Rules Heel Height: The ideal height is between 3 and 5 cm (1.2 to 2 inches). Contrary to popular belief, completely flat shoes on hard surfaces can cause plantar fasciitis. However, walking barefoot on soft surfaces (sand or grass) is highly beneficial. Cushioning: Look for soles and midsoles that provide adequate shock absorption to protect your knees and back. Width and Length: Your toes should be able to move freely. Avoid narrow “pointy” shoes that crush the toes together. Material: Prioritize natural, breathable materials like leather, linen, or organic cotton. Avoid rigid synthetics. Expert Tips to Reduce Damage Pelvic Floor Training: Use Kegel exercises or biofeedback devices to regain muscle tone. Strengthen Your Core: Practice Yoga, Pilates, or swimming. Avoid high-impact sports if you already suffer from pelvic hypertonia. Foot Hygiene: Use specific podiatric creams to nourish the skin rather than harsh exfoliants that can leave the foot vulnerable to infection. Self-Massage: Massage your legs from the feet upward to the hips twice a day using a “cold effect” gel to stimulate circulation. Active Stretching: Regularly stretch your calves and Achilles tendons to counteract the shortening caused by heels. Conclusion: Reclaiming Your Movement The phrase “Give a girl the right shoes and she can conquer the world” is often attributed to Marilyn Monroe. But “right” shouldn’t mean “painful.” From Sarah Jessica Parker, who admitted to permanent foot damage from years of wearing stilettos, to stars like Julia Roberts who have walked red carpets barefoot in protest, the tide is turning. Feminist icons like Germaine Greer have long labeled high heels as symbols of physical restriction. It’s time to rebel against footwear that destroys our health. Choose shoes that empower your movement, not shoes that hold you back. Choose the right shoes, and truly conquer the world. Source link

Can Stress Cause Hair Loss? Telogen Effluvium
We hear this all the time in the clinic. Someone comes in, visibly shaken, holding a clump of hair they found in the shower drain. “I’ve been under so much stress lately,” they say. “Could that actually be doing this?” The answer is yes. And the explanation is both more specific and more reassuring than most people expect. Let’s talk about what’s really happening. The Condition Has a Name: Telogen Effluvium Telogen effluvium (TE) is one of the most common forms of hair loss, and also one of the most misunderstood. It shows up as widespread shedding across your entire scalp rather than in patches or along a specific hairline. The part that catches most people off guard is the timing. It typically begins two to three months after whatever triggered it. So by the time your hair starts falling out, the stressful event may already feel like old news. According to NIH StatPearls, telogen effluvium happens when your body experiences significant stress and responds by pushing a large number of hair follicles out of the active growing phase and into a resting phase early. After sitting in that resting phase for about three months, those hairs shed all at once. That’s the sudden wave of shedding that brings so many people through our doors. Your Hair Has a Growth Cycle Here’s something most people never learn: every single hair on your head is on its own schedule, cycling through three phases continuously. The growing phase lasts two to seven years. The transitional phase lasts a couple of weeks. The resting phase lasts about three months, after which the hair naturally sheds and the follicle starts fresh. Under normal conditions, about 85 to 90 percent of your hair is actively growing at any point in time. When stress intervenes and throws a large group of follicles into the resting phase at the same time, you end up with far more shedding than usual all at once. That’s the shift from everyday hair loss to something that feels alarming. Source link
Navigating Life with POTS: My Dystautonomia Experience
Living with POTS (Dysautonomia) is new for me. Living with Migraine is something I’ve been living with forever. The thought that I live with something other than migraine has been a topic of discovery for many years. I know comorbidities are common with migraine so it’s been on my mind. Living with a chronic illness is complex because so much of it crosses over. My Migraine Life started way back when I was 5 years old. Over the last decade, I have dedicated my life to being a migraine advocate and educating myself about my disease. The pieces just weren’t coming together. For some reason, I felt like my migraine treatment was effective yet I was still in a chronic state of riding these intense symptoms that I couldn’t shake and came in flairs. This post is for informational purposes only, and should not be taken as medical advice in any way. Please speak with your doctor if you suspect you have dysautonomia and for treatment options. I am sharing my journey and everyone is different. Key Features of POTS Postural Orthostatic Tachycardia Syndrome (POTS) is a condition that affects the autonomic nervous system, which controls involuntary functions like heart rate, blood pressure, and digestion. POTS is a form of dysautonomia, and its primary characteristic is an abnormal increase in heart rate when transitioning from lying down to standing. Symptoms of POTS/Dysautonomia may Include: Heart rate: Fast or slow heart rate, heart palpitations, or an irregular heart rhythm Blood pressure: Low blood pressure, especially when standing up, or unstable blood pressure Blood sugar: Low blood sugar (hypoglycemia) Sweating: Excessive sweating, sweating more in certain areas, or not being able to sweat Temperature: Sensitivity to heat or cold, or swings in body temperature Vision: Blurred vision, light sensitivity, or trouble adjusting to light changes Headaches: Migraines or frequent headaches Dizziness: Frequent dizziness, especially when standing up Fainting: Fainting or passing out, especially when standing up Nausea and vomiting: Nausea and vomiting, or gastroesophageal reflux Bowel movements: Constipation or diarrhea, or changes in bowel movements Urination: Frequent urge to urinate, urinary incontinence, or bladder dysfunction Fatigue: Chronic fatigue or feeling tired all the time Cognitive issues: Brain fog, forgetfulness, or trouble concentrating Chest pain: Chest pain or discomfort Sleeping problems: Insomnia or sleep-disordered breathing Skin: Clammy or pale skin, blotchy reddening of the skin, or swelling and/or discoloration of the legs Dysautonomia Triggers: Prolonged standing, heat, dehydration, or illness can worsen symptoms. Hormonal changes, stress, or certain medications may also exacerbate the condition. What Causes POTS? The exact cause isn’t fully understood, but potential contributors include: Underlying Conditions: Viral illnesses or infections Autoimmune disorders (e.g., Sjögren’s syndrome, lupus) Ehlers-Danlos syndrome (a connective tissue disorder) Neuropathic POTS: Damage to small fiber nerves that regulate blood vessel constriction. Hyperadrenergic POTS: Excessive release of norepinephrine, leading to heightened “fight or flight” responses. Hypovolemic POTS: Low blood volume contributing to symptoms. Who Does It Affect? POTS is more common in women (80–85% of cases) and typically starts between the ages of 15 and 50. It can occur after a triggering event like a viral illness, surgery, pregnancy, or trauma. Is There a Cure for POTS? There’s currently no cure for POTS, but many treatments and lifestyle changes can significantly improve quality of life. My Diagnosis of POTS My diagnosis of POTS (postural orthostatic tachycardia syndrome /dysautonomia) was a long time coming. Chronic migraine allowed me to ignore other symptoms because my migraine symptoms are so diverse and range in intensity. One symptom I ignored was a burning in my leg which turned out to be blood pooling or neuropathic pain. I had this burning in my leg that I felt at night that went on for months, maybe even longer. It wasn’t something I thought to discuss with my headache specialist. It didn’t seem migraine-related and didn’t weigh heavy on my mind but it was something I mentioned to my husband often questioning what it could be. Looking back, this was a symptom of Neuropathic POTS and was a puzzle piece I put together in hindsight. A symptom I was talking about but possibly incorrectly was my anxiety. I was passing off my racing heart, clenching chest, and breathlessness on anxiety. My anxiety (or what I felt was anxiety) has been increasing in the last few years. Between living with chronic migraine and the stresses of life, my anxiety was through the roof and I didn’t consider blood pressure or heart rate to be something to discuss with my doctor. It was when I mentioned my head pain spiking when I was lying on the couch and walking upstairs to go to bed that my doctor mentioned POTS. Additionally, I was waking up with a migraine attack (or many symptoms of it) every morning. Even with a sleep schedule, when I went from lying to standing, my symptoms spiked. How Do I Know If I Have POTS? I had heard of POTS or dysautonomia at this point but was curious to have something to investigate further. I follow other migraine advocates who also speak about POTS and it’s comorbidity, like fibromyalgia or other conditions that often occur. It was something I never investigated. My headache specialist ordered a tilt test for me and a few weeks later I was standing there waiting to trigger my symptoms. I wasn’t sure how to feel. I have had many years of trying to figure out what else is going on besides migraine. Like migraine isn’t enough. I spent one summer between school and college and they were insistent that I had anemia because no one could figure out my dizziness. In 2018, I went to the Miles for Migraine Cincinnati race and met an amazing doctor who specializes in high/low-pressure headaches. When my doctor suggested it, I drove 4 hours to see this doctor to hear that I have both high and low-pressure headaches and it’s not that. But I escaped a painful test to discover this so that was a relief. Fast forward to 2023 and I’m still complaining of a spike of symptoms
Should gastroenterologists prescribe GLP-1s to their patients?
Column Editorials Add topic to email alerts Receive an email when new articles are posted on Please provide your email address to receive an email when new articles are posted on . “ data-action=”subscribe”> Subscribe We were unable to process your request. Please try again later. If you continue to have this issue please contact customerservice@slackinc.com. Back to Healio More from Column Editorials View all This month’s Healio Exclusive in Healio Gastroenterology poses a highly topical question. GLP-1 receptor agonists have revolutionized the treatment of obesity and related conditions, including type 2 diabetes, major adverse cardiovascular events, obstructive sleep apnea, metabolic dysfunction-associated steatotic liver disease, osteoarthritis and polycystic ovarian syndrome. The benefits of this drug class seem to far outweigh adverse events, which are often gastrointestinal. For some patients, including those with MASLD, gastroesophageal reflux disease or inflammatory bowel disease, there is evidence that these drugs may provide benefit. I personally have witnessed significant improvement in gastrointestinal symptoms for some of my patients with Crohn’s disease, ulcerative colitis and ileoanal pouch dysfunction. Furthermore, given the association between BMI and risk for gastrointestinal cancers, use of GLP-1s may prevent these malignancies. This raises the question: Should gastroenterologists prescribe these drugs as well? GLP-1s often seem to be under the purview of endocrinologists, weight management specialists or primary care providers. In one camp, we hear from gastroenterologists who subspecialize in obesity and feel we should fully embrace this drug class and be comfortable prescribing them. However, we also hear concerns about how GLP-1s are being marketed directly to patients through online health platforms, leading to little or no oversight of the prescription. One could argue this is a sign of primary care provider shortage and another reason for gastroenterologists to take ownership of prescribing GLP-1s. Given the broad number of indications for these drugs, it may be best for the primary care provider to “be the quarterback” and handle the prescribing. Certainly, gastroenterologists should embrace drugs such as tirzepatide and semaglutide in the sense that they should encourage patients with overweight or obesity to try them when the question is raised. As mentioned by Michael Camilleri, MD, DSc, in the cover story, use of GLP-1s fits nicely within the spectrum of treatments that should be offered to these patients after diet and lifestyle modifications but before endoscopic or surgical bariatric procedures. We also should be familiar with and comfortable discussing potential side effects of these medications, which include nausea, vomiting, diarrhea, constipation, indigestion, abdominal pain, fatigue and belching. We can talk patients through some of these side effects and reassure them that generally, they ease with time. We also should be aware of less common and more severe side effects such as biliary problems, pancreatitis and allergic reactions. Ultimately, the decision for a gastroenterologist to prescribe GLP-1s is a personal one and will depend on their patients and the availability of primary care providers who are comfortable with this class of drugs. Further research into the effect of the use of this drug class on gastrointestinal cancer prevention is warranted, too. For more information: Edward V. Loftus Jr., MD, is the Maxine and Jack Zarrow Family Professor of Gastroenterology at the Mayo Clinic and chief medical editor of Healio Gastroenterology. He can be reached at loftus.edward@mayo.edu. More from Column Editorials View all Published by: Sources/Disclosures Source: Expert submission Disclosures: Loftus reports consulting for AbbVie, Alvotech, Amgen, Boehringer Ingelheim, Bristol Myers Squibb, Celltrion Healthcare, Eli Lilly & Co., Fresenius Kabi, Gilead Sciences, Janssen and Takeda Pharmaceuticals; and receiving research support from AbbVie, Bristol Myers Squibb, Celgene/Receptos, Gilead, Janssen and Takeda. Ask a clinical question and tap into Healio AI’s knowledge base. PubMed, enrolling/recruiting trials, guidelines Clinical Guidance, Healio CME, FDA news Healio’s exclusive daily news coverage of clinical data Learn more Add topic to email alerts Receive an email when new articles are posted on Please provide your email address to receive an email when new articles are posted on . “ data-action=”subscribe”> Subscribe We were unable to process your request. Please try again later. If you continue to have this issue please contact customerservice@slackinc.com. Back to Healio Source link

Get Active This Spring with Low-Impact Exercises for Pain Relief and Better Mobility
Preventing Winter Falls: Balance and Strength Training Tailored for Cold Weather Challenges By Bob Berendsen • January 15, 2026 Winter, widely considered the season of comfort, is the time for indoor relaxation and quiet contemplation. However, winter also brings with it some very real dangers, including cold, dark, and slippery surfaces. For older adults or those dealing with chronic pain, a small slip on these surfaces can lead to serious injuries that take months to heal. The good news? You can train your body to handle these challenges. Let’s explore some simple, safe exercises you or your loved ones can do from the comfort of your home to build your winter-proof stability. Why Winter Increases the Risk of Falls Cold weather brings more than just chilly air. It changes the way we move, how our muscles respond, and even how we think about walking. When it’s icy, people tend to tense up, take shorter steps, and look down more often. Muscles also get tighter in the cold, which reduces flexibility. Plus, all those bulky layers of clothes mess with your center of gravity and limit how quickly you can react if you start to lose your balance. Your boots might be waterproof and warm, but they’re probably not giving you the ankle support or ground feel you’d get from your regular shoes. Then there’s the simple fact that many of us move less in winter. Maybe you skip your daily walks when it’s freezing, or you stop going to that exercise class because driving feels too risky. But here’s the catch: the less you move, the weaker you get, and the weaker you get, the more likely you are to fall. Building a Foundation To prevent this, you simply need to work on two main things: balance and strength. Physical therapy and balance-focused exercises train your muscles, joints, and nervous system to respond faster and more effectively when something throws you off. Balance Training Balance isn’t just about standing still without wobbling. It’s about how your body reacts when something throws it off center. When you step on ice, for example, your brain and muscles have to communicate in an instant to keep you upright. If that connection is slow or weak, you’re more likely to fall. Some simple ways to train your balance include: ● Single Leg Stands : Stand near a sturdy surface like a countertop or wall for support. Lift one foot slightly off the ground and hold that position for 10–15 seconds. Then switch sides. At first, you might wobble, but that’s perfectly normal. Over time, your legs, ankles, and core muscles will get stronger, and your balance will improve. Try doing 3 rounds on each leg daily. ● Heel-to-Toe Walk: Imagine you’re walking on a tightrope. Place one foot directly in front of the other, heel touching toe, as you move slowly across the room. This simple drill strengthens your stabilizing muscles and sharpens coordination. Keep your eyes forward, not down, and use a wall for light support if needed. ● Side Leg Raises: Hold onto a sturdy chair or counter. Lift one leg out to the side while keeping your back straight and your toes facing forward. Lower it slowly and repeat. This exercise builds hip strength, which plays a big role in staying upright on slippery ground. ● Weight Shifts: Stand with your feet hip-width apart and shift your weight from one leg to the other slowly. Feel your balance change from left to right. This gentle exercise teaches your body to adjust quickly. Strength Training Balance and strength go hand in hand. When your muscles are strong, they act like shock absorbers, keeping you stable even when your footing isn’t perfect. Focus on the muscles that support your posture and help you move safely. Here are a few simple exercises to include in your daily routine: ● Chair Squats: Sit down and stand up from a sturdy chair without using your hands for support. Keep your feet flat on the floor and your knees aligned with your toes. This move strengthens your thighs, hips, and glutes—key muscles for stability and control. ● Heel Raises: Stand behind a chair or counter and slowly lift your heels so you’re standing on your toes. Lower back down after holding for a few seconds. This helps strengthen your calves and ankles, improving the small muscle reactions that keep you upright when you slip. ● March in Place: Lift your knees high as if you’re marching. Do this for one to two minutes, rest, and repeat. Marching builds leg endurance and helps train your coordination. ● Core Squeezes: While sitting or standing, tighten your stomach muscles as if you’re zipping up a snug jacket. Hold for 10 seconds, then release. A strong core helps your upper and lower body work together to keep you balanced. These movements may look simple, but they’re powerful. Doing them for just 10–15 minutes a day can make winter walks safer and less stressful. Warming Up Before You Head Outdoors Cold weather tightens muscles and slows blood flow, making your body less responsive. That’s why warming up before heading outside is so important. Think of it as insurance against sudden slips. Try a short warm-up routine before stepping out: ● Arm circles to loosen shoulders. ● Gentle knee bends to wake up leg muscles. ● Shoulder rolls and neck stretches to improve mobility. ● A quick indoor walk or stair climb to raise your heart rate slightly. It’s also wise to check your footwear. Look for rubber soles with deep treads for better traction. Avoid smooth or worn-out shoes, and consider ice grips that attach to your boots if you live in a particularly snowy area. Winter doesn’t have to be a season of fear. By investing just 10-15 minutes a day in these simple, safe exercises, you can build the strength and confidence you need to navigate the season safely. You are giving your body the tools it needs to

Heather se hace una prueba del VIH
[GRAPHIC] Heather, una mujer de casi 60 años, sostiene su teléfono y su aplicación de citas muestra que alguien que le gusta quiere conocerla. Tiene una enorme sonrisa en su rostro mientras aparece un globo de diálogo que muestra su conversación. Hombre: “¿Cenamos el viernes en la noche?” Heather: “¡Es una cita!” [GRAPHIC] Heather está en su cita, ella y él están sentados juntos y él tiene su brazo sobre los hombros de Heather. Hombre: “¿Vamos a otro lugar?” Heather: “¿Tu casa o la mía?” [SUPER] Días después… [GRAPHIC] Heather y su amiga están sentadas en el sofá en la casa de Heather. Mientras conversan, ambas sostienen vasos de vino, comen bocadillos, acarician un gato, etcétera. Amiga: “¡Cuéntame cómo te fue en tu cita!” Heather: “Estuvo bien. Ya sabes, no busco nada serio. Solo deseo divertirme mientras conozco gente nueva después del divorcio. Tener citas a los 56 años ha sido una aventura”. Amiga: “¿Y qué pasó con Brad? ¿Todavía se ven?” Heather: “Nos vemos casualmente”. Amiga: “Epa, estoy viviendo todo esto a través de ti. Por cierto, ¿qué haces para protegerte? ¿Todavía tomas píldoras anticonceptivas?” Heather: “No, dejé de tomarlas hace varias semanas. Lo bueno de la menopausia es que no tienes que preocuparte de embarazarte. ¡Qué alivio!” Amiga: “¿Y cómo te proteges de ITS (infecciones de transmisión sexual)?” Heather: “Eso no me preocupa mucho”. Amiga: “No deseo desanimarte, pero puesto que soy enfermera, siento que debo decirte que las tasas de ITS están aumentando. Se duplicaron para personas de entre los 50 y 60 años en la última década”. Heather: “¿Por qué?” Amiga: “Algo de eso se debe a personas como tú, que están volviendo a salir con parejas nuevas después de un divorcio, pensando que ya no necesitan protección. Y la menopausia en sí puede hacerte más propensa a enfermarte de ITS”. Heather: “Epa, qué sorpresa. La menopausia realmente es un regalo que nunca acaba”. [GRAPHIC] Cambios vaginales, tales como la pérdida de elasticidad y sequedad, te hacen más propensa a laceraciones, lo cual hace que sea más fácil enfermarse de ITS. Amiga: “Tal vez deberías hacerte una prueba del VIH. Solo por seguridad”. Heather: “Eso me da miedo”. Amiga: “Es una simple prueba de sangre. Y no saber tu situación da más miedo, ¿no lo crees así? Heather: “Supongo que sí. Tienes razón”. [ SUPER] Puedes hacerte una prueba del VIH en: El consultorio de tu proveedor médico Un departamento de salud pública local Clínicas con pruebas del VIH Amiga: “Si tienes el VIH y recibes tratamiento, todavía podrás disfrutar de una vida larga y saludable. Pero si ignoras algo así, podría ser mortal”. Heather: “Gracias. Siempre me das buenos consejos. ¡Lo haré! Encontraré un lugar mañana. Ahora enfoquémonos en el evento principal de la noche. Veamos ‘¡El amor es ciego!’” Source link


