

Preventing Winter Falls: Balance and Strength Training Tailored for Cold Weather Challenges By Bob Berendsen • January 15, 2026 Winter, widely considered the season of comfort, is the time for indoor relaxation and quiet contemplation. However, winter also brings with it some very real dangers, including cold, dark, and slippery surfaces. For older adults or those dealing with chronic pain, a small slip on these surfaces can lead to serious injuries that take months to heal. The good news? You can train your body to handle these challenges. Let’s explore some simple, safe exercises you or your loved ones can do from the comfort of your home to build your winter-proof stability. Why Winter Increases the Risk of Falls Cold weather brings more than just chilly air. It changes the way we move, how our muscles respond, and even how we think about walking. When it’s icy, people tend to tense up, take shorter steps, and look down more often. Muscles also get tighter in the cold, which reduces flexibility. Plus, all those bulky layers of clothes mess with your center of gravity and limit how quickly you can react if you start to lose your balance. Your boots might be waterproof and warm, but they’re probably not giving you the ankle support or ground feel you’d get from your regular shoes. Then there’s the simple fact that many of us move less in winter. Maybe you skip your daily walks when it’s freezing, or you stop going to that exercise class because driving feels too risky. But here’s the catch: the less you move, the weaker you get, and the weaker you get, the more likely you are to fall. Building a Foundation To prevent this, you simply need to work on two main things: balance and strength. Physical therapy and balance-focused exercises train your muscles, joints, and nervous system to respond faster and more effectively when something throws you off. Balance Training Balance isn’t just about standing still without wobbling. It’s about how your body reacts when something throws it off center. When you step on ice, for example, your brain and muscles have to communicate in an instant to keep you upright. If that connection is slow or weak, you’re more likely to fall. Some simple ways to train your balance include: ● Single Leg Stands : Stand near a sturdy surface like a countertop or wall for support. Lift one foot slightly off the ground and hold that position for 10–15 seconds. Then switch sides. At first, you might wobble, but that’s perfectly normal. Over time, your legs, ankles, and core muscles will get stronger, and your balance will improve. Try doing 3 rounds on each leg daily. ● Heel-to-Toe Walk: Imagine you’re walking on a tightrope. Place one foot directly in front of the other, heel touching toe, as you move slowly across the room. This simple drill strengthens your stabilizing muscles and sharpens coordination. Keep your eyes forward, not down, and use a wall for light support if needed. ● Side Leg Raises: Hold onto a sturdy chair or counter. Lift one leg out to the side while keeping your back straight and your toes facing forward. Lower it slowly and repeat. This exercise builds hip strength, which plays a big role in staying upright on slippery ground. ● Weight Shifts: Stand with your feet hip-width apart and shift your weight from one leg to the other slowly. Feel your balance change from left to right. This gentle exercise teaches your body to adjust quickly. Strength Training Balance and strength go hand in hand. When your muscles are strong, they act like shock absorbers, keeping you stable even when your footing isn’t perfect. Focus on the muscles that support your posture and help you move safely. Here are a few simple exercises to include in your daily routine: ● Chair Squats: Sit down and stand up from a sturdy chair without using your hands for support. Keep your feet flat on the floor and your knees aligned with your toes. This move strengthens your thighs, hips, and glutes—key muscles for stability and control. ● Heel Raises: Stand behind a chair or counter and slowly lift your heels so you’re standing on your toes. Lower back down after holding for a few seconds. This helps strengthen your calves and ankles, improving the small muscle reactions that keep you upright when you slip. ● March in Place: Lift your knees high as if you’re marching. Do this for one to two minutes, rest, and repeat. Marching builds leg endurance and helps train your coordination. ● Core Squeezes: While sitting or standing, tighten your stomach muscles as if you’re zipping up a snug jacket. Hold for 10 seconds, then release. A strong core helps your upper and lower body work together to keep you balanced. These movements may look simple, but they’re powerful. Doing them for just 10–15 minutes a day can make winter walks safer and less stressful. Warming Up Before You Head Outdoors Cold weather tightens muscles and slows blood flow, making your body less responsive. That’s why warming up before heading outside is so important. Think of it as insurance against sudden slips. Try a short warm-up routine before stepping out: ● Arm circles to loosen shoulders. ● Gentle knee bends to wake up leg muscles. ● Shoulder rolls and neck stretches to improve mobility. ● A quick indoor walk or stair climb to raise your heart rate slightly. It’s also wise to check your footwear. Look for rubber soles with deep treads for better traction. Avoid smooth or worn-out shoes, and consider ice grips that attach to your boots if you live in a particularly snowy area. Winter doesn’t have to be a season of fear. By investing just 10-15 minutes a day in these simple, safe exercises, you can build the strength and confidence you need to navigate the season safely. You are giving your body the tools it needs to

Heather Gets an HIV Test
[SUPER] Later that week… [GRAPHIC] Heather and her friend are sitting on the couch at Heather’s house. Throughout the conversation, they are both holding glasses of wine, eating snacks, petting a cat, etc. Friend: “So tell me about the date!” Heather: “It was alright. You know me, I’m not looking for anything serious. Just having fun getting back out there since the divorce. Dating at 56 has been an adventure so far.” Friend: “And what about Brad? Are you still seeing him?” Heather: “Casually.” Friend: “Wow, I’m totally living vicariously through you. By the way, what are you doing for protection? Are you still on the pill?” Heather: “No, I got off that a few weeks ago. One good thing about menopause is that you don’t have to worry about getting pregnant. Whew!” Friend: “But what about STIs?” Heather: “I’m not too worried.” Friend: “Not to put a chill on Netflix and chill, but since I’m a nurse, I feel like I need to tell you that STIs are actually on the rise. They’ve doubled in people in their mid-50s and older in the last decade.” Heather: “Really? Why?” Friend: “Some of it is from people like you, who are getting back out there with new partners after a divorce, thinking they no longer need protection. And menopause itself can make you more likely to get STIs.” Heather: “Oh, wow. Menopause really is the gift that keeps on giving.” [GRAPHIC] Changes in the vagina, like loss of elasticity and dryness, make you more prone to tearing, which makes it easier to get STIs. Friend: “Maybe you should get an HIV test. Just to be safe.” Heather: “That sounds scary.” Friend: “It’s really just a simple blood test. And not knowing is a lot scarier though, right? Heather: “I guess. Yeah.” [ SUPER] You can get an HIV test at: Your healthcare provider’s office Local health departments HIV testing clinics Friend: “If you have HIV and you get treated, you can still live a long, healthy life. But if you ignore something like that, it can be life-threatening.” Heather: “Thanks. You always give me good advice. I’ll do it! I’ll find a place tomorrow. Now let’s get to the main event of the evening. Turn on “Love Is Blind!” Source link

69 Sex Positions You Need to Try
If you purchase an independently reviewed product or service through a link on our website, SheKnows may receive an affiliate commission. No shade at your tried-and-true sex positions—after all, hopefully, they’ve become faves for good reasons, like consistent climax and connection. The thing is, with so many pleasurable sexual configurations to try, there’s really no good reason not to branch out while you bone. Not to mention, trying new sex positions can help stoke the so-called sexual flames, keeping things hot-hot-hot even as the months and years go on. Of course, things like new sex toys (our personal favorite is LELO’s award-winning Enigma Double Sonic) can help heat things up too. There are plenty of ways to make sure that no two nights in are exactly the same, whether you’re playing solo or with a partner or two. Sometimes all it takes is a brand-spanking-new position to get the party started and to reignite some important conversations about what feels best in the act. (And remember, it’s okay if those things change or if you just want to test something out!) We also know you’re busy and probs don’t want to waste precious time researching impossible pretzel-like contortions. That’s why we asked queer sex educator and sex journalist Gabrielle Kassel to share the best sex positions for reigniting the spark, whether you’re playing solo or with a partner or two. Read on for a compilation of 69 (nice) sexpert-based sex positions we think you should try ASAP. A version of this story was originally published in July 2016. Pin it! Image Credit: Adobe Stock/New Africa Pin now, try them out later! Classic Sex Positions Modified Coital-Alignment Technique Image Credit: Ashley Britton/SheKnows Essentially an upgraded version of missionary, the Coital Alignment Technique position (aka CAT) is a face-to-face position that involves the penetrating partner moving up and down rather than in and out. For this elevated variation, the receiving partner lays on their back. Then, the penetrating partner enters from above. The key word here? Above. The penetrating partner needs to shift their weight forward so that their penis or dildo presses all along the external vulva rather than going right for the glory holes. Why It’s Great: Once in position, the penetrator should avoid thrusting and instead focus on moving their hips in circles. This simultaneously massages the internal erogenous zones in the vagina (like the G-spot) as well the clitoral glans. Meanwhile, the receiving partner should experiment with tilting their hips at various angles, as well as wrapping their legs around their lover’s back. Doggy Style Image Credit: Ashley Britton/SheKnows As far as rear-entry sex positions go, doggy style is top dog. For this classic, the receiving partner gets on all fours while the penetrating partner stands or kneels behind them and goes to town. From here, the receiving partner can ‘cat-cow’ their pelvis to facilitate pressure against their most sensitive hot-spots, while the penetrating partner can use their hands to grip, grab, or grope to their heart’s content. Why It’s Great: On the physical front, the doggy style allows for easy to the G-spot (shallow penetration) or A-spot (deeper penetration), depending on the exact angle. Plus, the receiving partner is perfectly positioned to stimulate their clit with their hand or vibe. Meanwhile, emotionally and mentally, the bestial position can be arousing because it often feels more intense and less restrained. Not to mention, there are a lot of modifications to give the giver and receiver something they’ll enjoy, such as anal doggy, flat doggy, and wheelbarrow. Pushing Tush Image Credit: Ashley Britton/SheKnows Butt-lovers rejoice! The Pushing Tush, sometimes known as rear-entry missionary, is a sex position that makes the back door the star of the show. You’ll assume the missionary position, but rather than the vagina being the point of entry, the anus will be. To facilitate the angle of entry, the bottom partner should put a sex pillow under their hips. Alternatively, the bottom can plant their feet into the mattress and then actively tilt their hips up and press their spine into the ground, which will open the anal canal. In case it needs to be said, lube is an absolute must here. The anal canal is never self-lubricating in the way the vagina often is. So, to reduce uncomfortable friction and facilitate that feel-good slide-and-glide, you’ll want to lather the insertive body part or toy with lubricant and use a lube shooter to coat the inner canal. Why It’s Great: This is a solid choice if either partner has expressed interest in playing around with anal penetration in an intimate way. A suitable position for both anal with a penis and dildo (aka pegging), this face-to-face position allows the penetrating partner to read their partner’s facial cues for additional insight on comfort. If both partners want to enjoy anal penetration at the same time, consider having the top partner plop in a vibrating butt plug or prostate massager ahead of entry. Rocking Horse Image Credit: Ashley Britton/SheKnows The Rocking Horse will become your new fave for G-spot stimulation and intimate eye-contact. In this position, the receiving partner sits between the penetrating partner’s legs, with the receiving partner’s legs just short of wrapped around them (but you can modify for that if you want to go full Koala!). Why It’s Great: With Rocking Horse, both partners rock into each other, which gives you a lot of room to control the depth of penetration while also holding each other super close. It can be as gentle or as sexy (or a combo of both!) as you like. Seated Scissors Image Credit: Ashley Britton/SheKnows Think of seated scissors as a play on reverse cowgirl — and we mean play, because this position is a fun one. The penetrating partner lies on their back with one leg bent while the receiving partner gets on top, straddling their bent leg and arranging their legs however feels comfortable. There’s plenty of support up top and lots of room for both partners to
Hair Transplant Surgeons who also had Hair Transplants
A hair transplant surgeon getting a hair transplant. Far more common than you would expect. Around 25 years ago, I started bookmarking hair transplant surgeon websites if it was mentioned that the surgeon had also undergone a hair transplant himself. Later on, I wrote this post in 2014 and am now republishing it in case anyone has any updates. I only include names of relatively well known hair transplant focused surgeons who mention their own surgery on their website. I find it reassuring that there are so many hair transplant surgeons who have also had hair transplants themselves. Especially when they get the procedure at their own clinic, often at the hands of a partner. It shows that they have confidence in the process, the final results and in their own staff’s skills. Some of them also mention their own traumatic hair loss at a very young age being the reason for their passion in this field. A select few of these surgeons have before and after photos on their sites as evidence. Some only briefly point out the fact in their webpage text. Some used to mention their own hair transplant experiences, but later on removed the information during site updates. As is the case with hair restoration surgery patients, many surgeons likely prefer not posting personal before and after photos online. Or they might add but later remove such photos if they have had continuing major hair loss in the years after surgery. I would not be surprised if at least one-half of balding hair transplant surgeons in the world had not tested at least a small-scale procedure on their own scalp. Hair Transplant Surgeons who had Hair Transplants Themselves Dr. Edward Ball — On his site, it says that Dr. Ball underwent an FUE hair restoration procedure using the ARTAS® Robotic System. Dr. David Perez-Meza — Confirmed to me on Twitter. He had four strip (FUT) hair transplant surgeries between 1998 and 2007. Dr. Ken Williams — Per his website, he is the recipient of five FUE surgeries since 2009. He had over 10,000 grafts transplanted into his Norwood 5-6 hair loss pattern. Dr. Michael Beehner — There used to be some great before and after pictures on his site, but he might have retired now. Dr. Christopher Pawlinga — On his old site, it mentioned that his partner at the time (Dr. Beehner) did his hair transplant in 1994. Dr. Bradley Wolf — Was operated upon by the well known and highly respected surgeon Dr. Ron Shapiro. Dr. Wolf told me this when I met him once. Unfortunately, his website no longer has the before and after photos that it used to have. Dr. John Satino — He mentioned this to me over the phone and you can read more about this interesting personality in my post on PRP and hair darkening. He had a number of scalp reductions and hair transplants decades ago from the famous Dr. Constantine Chambers. Prior to his demise at the age of 80 in 2025, Dr. Satino still had great hair. Dr. Robert Jones — One of the case studies on his old homepage entailed his own hair transplant. He also wrote some interesting blog posts related to his own hair restoration procedures. This well known Toronto-based surgeon now seems to be retired. Dr. Gary Hitzig — His old site used to have that information. It seems like he no longer has a website and might have retired. Dr. Matt Leavitt — Founder of MHR (now merged with Bosley). His old site used to have his before and after photos. Dr. John Gillespie — This Calgary-based surgeon used to mention it on his old site, but he is now retired. Dr. Richard Rogers — Used to mention it. Dr. Alan Feller — His old site used to have that information. Dr. Robert Haber — I met him once and he told me that he had a hair transplant in the past. Dr. Robert Dorin — His partner Dr. Robert True performed his hair transplant. Dr. William Rassman — On his now defunct blog, he wrote a post describing his own crown hair transplant. Dr. Jerry Cooley — I think his old site used to have that info based on my bookmark. Dr. Brian Goertz — I met him in person once to get a Proscar prescription and he showed me his before and after photos. Now retired. Dr. Dan McGrath — Mentions it on his site. Dr. William Yates — His own hair transplant made a big difference in his confidence and life per his old site. A rare testimonial from an African American who hated his hair loss. He also got some beard hair to head transplants from Dr. John Cole. Dr. William Reed — Mentions that he got two hair transplantation procedures in 1994. Dr. Marc Dauer — I think his old site used to have that info based on my bookmark. Dr. Raghu Reddy — Has an excellent write-up with photos of his own experience with hair loss: a bad first hair transplant (including shock loss); and later on a good second FUE hair transplant by his own technician. Dr. Ken Washenik — Mentioned in the linked wired.com article. He is among the five most cited hair loss spokespersons in the world. Dr. Bessam Farjo — Scroll down the page for his thoughts on his unsuccessful hair transplants with old technology. Dr. Alan Bauman’s Father — Dr. Bauman might never need a hair transplant himself, but he did operate on his father with great results. Link no longer works so I remove it. Dr. Paul Spano — Mentioned it on an older site. Dr. Bernard Arocha — Mentioned on his site. Dr. Robert Leonard — In August 2014, after I wrote this post, Dr. Leonard posted photos on Twitter of his hair transplant. His partner Dr. Matthew Lopresti performed an FUE hair transplant on him using the ARTAS robot. Dr. Michael Vories — Mentions that he was a hair transplant patient prior to becoming a surgeon. Dr. Paul

The Migraine Trust joins leading organisations to shape government’s Keep Britain Working initiative
The Migraine Trust, alongside over 150 other employers, is working with the government to tackle ill-health that pushes many people with long-term health conditions and disabilities, like migraine, out of work. This group of organisations, called Vanguards, includes some of the biggest employers in the country, healthcare providers, mayoral authorities, and charities like The Migraine Trust. It has been assembled by the government as part of its Keep Britain Working programme following the publication of the Keep Britain Working Review in November 2025. The Vanguards will work with the government to help reshape how health issues and disabilities are managed in the workplace. They will contribute to the development of practical, scalable solutions across several aspects of the ‘healthy working lifecycle’, including improving disability inclusion, acting early to prevent deteriorating health at work and supporting employees to remain and return to work. The Migraine Trust is looking forward to working with the government and fellow employer Vanguards to ensure that the workplace needs of people living with migraine are represented. 33% had to leave their job altogether due to the impact of migraine We know from our research that many of the one in seven people living with migraine have experienced a significant impact on their employment because of the condition. Research we conducted in 2023 highlighted that a staggering 29% of people with migraine said they had needed to move from full-time to part-time work because of migraine, while 33% had to leave their job altogether. Employers have an important role to play in ensuring people with migraine are supported to stay in, and thrive at, work. According to our 2025 survey of people with migraine, only 2% of respondents strongly agreed that their workplace had migraine-friendly policies. Often, simple and straightforward changes in the workplace can make a big difference for people with migraine. Whether you are an employer, a colleague of someone with migraine, or you live with migraine yourself, our workplace hub has lots of resources and support, including details on how to book a migraine training session for your workplace. Source link
AI uses routine data to create biomarker for pancreatic cancer
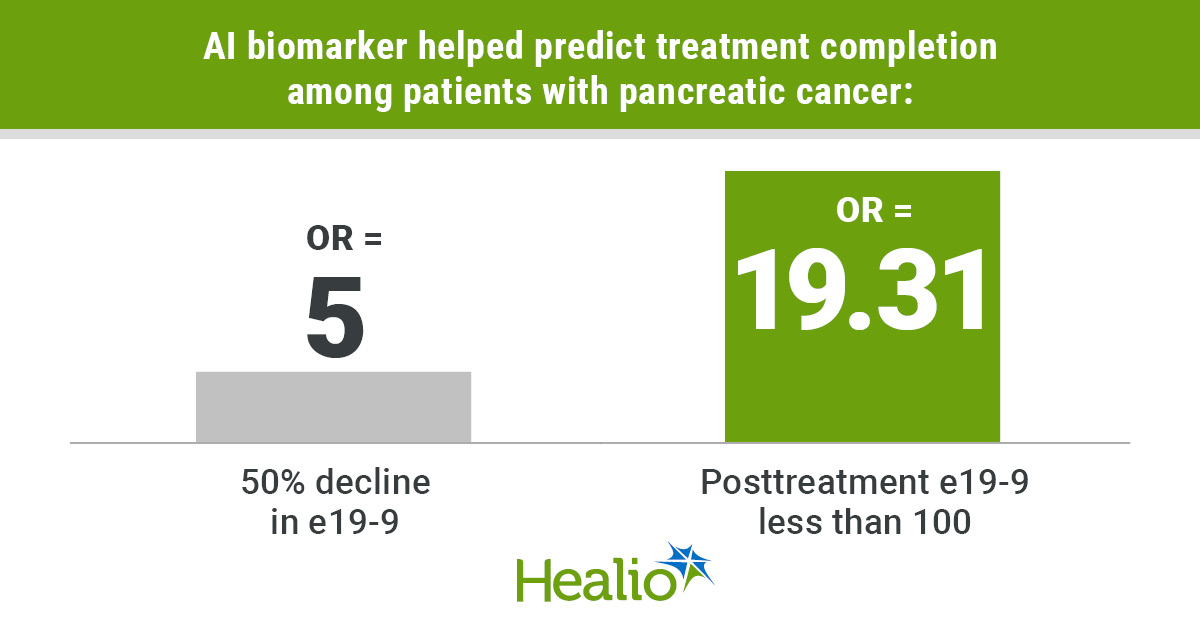
Add topic to email alerts Receive an email when new articles are posted on Please provide your email address to receive an email when new articles are posted on . “ data-action=”subscribe”> Subscribe We were unable to process your request. Please try again later. If you continue to have this issue please contact customerservice@slackinc.com. Back to Healio Key takeaways: About a third of patients do not have a biomarker used to track treatment progress in pancreatic cancer. An AI biomarker derived from routinely collected data predicted treatment completion and survival. Approximately a third of patients with pancreatic ductal adenocarcinoma do not have elevated or detectable levels of a biomarker commonly used to measure response to therapy. An AI tumor marker derived from routinely collected data could provide prognostic information on treatment completion and survival similar to that seen in patients who have measurable cancer antigen 19-9 (CA19-9). Data derived from Thalji SZ, et al. JAMA Surg. 2026;doi:10.1001/jamasurg.2026.0291. Anai N. Kothari “This behaves just like CA19-9 does clinically,” Anai N. Kothari, MD, MS, assistant professor of surgical oncology at Medical College of Wisconsin, told Healio. “It tracks response, predicts outcomes and can help guide treatment decisions. This really is a step forward using AI, not just to predict outcomes, but to fill in some critical gaps in clinical care using data we already have.” ‘A big gap’ Pancreatic ductal adenocarcinoma (PDAC) tumors can exhibit significant changes on imaging, so clinicians use biomarker CA19-9, a serum blood value, to measure response to therapy and make prognostic assessments, according to study background. However, about 30% of patients with PDAC do not produce elevated levels of CA19-9, including 10% who do not have any detectable CA19-9. “There’s no high-quality biomarker in that patient population to follow,” Kothari said. “Instead, [clinicians use] a lot of intermittent screening tests, imaging that ends up being costly and challenging for the patients to do. They may miss an opportunity to change treatment in someone who’s not responding. This is a big gap that needed to be filled.” Kothari and colleagues investigated whether AI could use other common laboratory data routinely collected along with CA19-9 to find a surrogate biomarker, which they called electronic CA19-9 (e19-9). They trained the model on 3,239 patients with PDAC and elevated C19-9. The cohort had a combined 21,555 unique CA19-9 values. Researchers then conducted external validation on 4,384 similar patients with 16,487 unique CA19-9 values. Finally, they tested the model on 121 patients with localized PDAC (median age, 65 years; interquartile range, 14; 51% men; 89% white) who did not have elevated CA19-9 (less than 35 U/mL). Completion of all neoadjuvant treatment and surgery, metastatic progression and OS served as primary endpoints. ‘Highly usable tool’ Overall, 77% of patients in the test cohort completed neoadjuvant therapy, including surgery. Individuals who finished treatment had similar e19-9 values before therapy as those who did not complete treatment (median, 121 vs. 134.1). Kothari and colleagues found patients who had at least a 50% decline in e19-9 during treatment had a significantly higher likelihood of finishing (OR = 5; 95% CI, 1.6-15.66). Additionally, patients who had posttreatment e19-9 levels less than 100 had nearly 20 times the likelihood of completing therapy, including surgery (OR = 19.31; 95% CI, 5.8-64.26). Metastatic progression occurred significantly less in patients who had any decline in e19-9 (47% vs. 80%; P = .01), those who had a 50% decrease (24% vs. 56%; P = .01), and those with levels less than 100 (29% vs. 80%; P < .001). OS significantly increased among patients who had any decline in e19-9 (median, 49 months vs. 22 months; P = .03), those with a 50% reduction (median, 53 months vs. 32 months; P = .007), and those with posttreatment levels less than 100 (median, 60 months vs. 16 months; P < .001). E19-9 less than 100 had a significant association with improved OS (HR = 0.49; 95% CI, 0.25-0.97). “This is a highly usable tool, and it sets the stage for a lot more innovation and impact by using AI the right and responsible way,” Kothari said. “Before, for this 30% of patients who have pancreas cancer, we didn’t have a reliable way of making these estimates over time. Now, the data show we have a biomarker for that 30%. We have something that can guide treatment decision-making, to look at things over the course of their therapy, and to be able to give them some idea of the probability that they would make it to surgery, or what their survival could look like.” Researchers acknowledged study limitations, including e19-9 being based on a predictive model. Kothari noted the importance of further prospective analysis at different institutions. He also highlighted the impact this could have on other malignancies. “Why stop at pancreas cancer?” he asked. “We know that tumor biomarkers are important parts of other cancers, and similar to the problem in pancreas cancer, there’s a subset of patients who don’t have a meaningful ability to use that biomarker. There are other populations we can help with this same methodology. The key is that we’re not drawing any new information, new labs. We’re just using the data we already have to be able to provide this information.” This is the benefit AI can provide. “I’ve been studying artificial intelligence for over a decade,” Kothari said. “There’s always this promise that AI was going to identify information that the human eye could not see. For an individual patient with cancer, we now gather up to a million data points as part of their treatment. We can use AI to see patterns, then augment that with our human expertise to improve not just cancer outcomes, but health outcomes overall. Instead of treating everyone exactly the same, we really are homing in on what’s personal and unique about that individual.” For more information: Anai N. Kothari, MD, MS, can be reached at akothari@mcw.edu. Published by:

Pain Flares: Why They Happen and How to Manage Them
Preventing Winter Falls: Balance and Strength Training Tailored for Cold Weather Challenges By Bob Berendsen • January 15, 2026 Winter, widely considered the season of comfort, is the time for indoor relaxation and quiet contemplation. However, winter also brings with it some very real dangers, including cold, dark, and slippery surfaces. For older adults or those dealing with chronic pain, a small slip on these surfaces can lead to serious injuries that take months to heal. The good news? You can train your body to handle these challenges. Let’s explore some simple, safe exercises you or your loved ones can do from the comfort of your home to build your winter-proof stability. Why Winter Increases the Risk of Falls Cold weather brings more than just chilly air. It changes the way we move, how our muscles respond, and even how we think about walking. When it’s icy, people tend to tense up, take shorter steps, and look down more often. Muscles also get tighter in the cold, which reduces flexibility. Plus, all those bulky layers of clothes mess with your center of gravity and limit how quickly you can react if you start to lose your balance. Your boots might be waterproof and warm, but they’re probably not giving you the ankle support or ground feel you’d get from your regular shoes. Then there’s the simple fact that many of us move less in winter. Maybe you skip your daily walks when it’s freezing, or you stop going to that exercise class because driving feels too risky. But here’s the catch: the less you move, the weaker you get, and the weaker you get, the more likely you are to fall. Building a Foundation To prevent this, you simply need to work on two main things: balance and strength. Physical therapy and balance-focused exercises train your muscles, joints, and nervous system to respond faster and more effectively when something throws you off. Balance Training Balance isn’t just about standing still without wobbling. It’s about how your body reacts when something throws it off center. When you step on ice, for example, your brain and muscles have to communicate in an instant to keep you upright. If that connection is slow or weak, you’re more likely to fall. Some simple ways to train your balance include: ● Single Leg Stands : Stand near a sturdy surface like a countertop or wall for support. Lift one foot slightly off the ground and hold that position for 10–15 seconds. Then switch sides. At first, you might wobble, but that’s perfectly normal. Over time, your legs, ankles, and core muscles will get stronger, and your balance will improve. Try doing 3 rounds on each leg daily. ● Heel-to-Toe Walk: Imagine you’re walking on a tightrope. Place one foot directly in front of the other, heel touching toe, as you move slowly across the room. This simple drill strengthens your stabilizing muscles and sharpens coordination. Keep your eyes forward, not down, and use a wall for light support if needed. ● Side Leg Raises: Hold onto a sturdy chair or counter. Lift one leg out to the side while keeping your back straight and your toes facing forward. Lower it slowly and repeat. This exercise builds hip strength, which plays a big role in staying upright on slippery ground. ● Weight Shifts: Stand with your feet hip-width apart and shift your weight from one leg to the other slowly. Feel your balance change from left to right. This gentle exercise teaches your body to adjust quickly. Strength Training Balance and strength go hand in hand. When your muscles are strong, they act like shock absorbers, keeping you stable even when your footing isn’t perfect. Focus on the muscles that support your posture and help you move safely. Here are a few simple exercises to include in your daily routine: ● Chair Squats: Sit down and stand up from a sturdy chair without using your hands for support. Keep your feet flat on the floor and your knees aligned with your toes. This move strengthens your thighs, hips, and glutes—key muscles for stability and control. ● Heel Raises: Stand behind a chair or counter and slowly lift your heels so you’re standing on your toes. Lower back down after holding for a few seconds. This helps strengthen your calves and ankles, improving the small muscle reactions that keep you upright when you slip. ● March in Place: Lift your knees high as if you’re marching. Do this for one to two minutes, rest, and repeat. Marching builds leg endurance and helps train your coordination. ● Core Squeezes: While sitting or standing, tighten your stomach muscles as if you’re zipping up a snug jacket. Hold for 10 seconds, then release. A strong core helps your upper and lower body work together to keep you balanced. These movements may look simple, but they’re powerful. Doing them for just 10–15 minutes a day can make winter walks safer and less stressful. Warming Up Before You Head Outdoors Cold weather tightens muscles and slows blood flow, making your body less responsive. That’s why warming up before heading outside is so important. Think of it as insurance against sudden slips. Try a short warm-up routine before stepping out: ● Arm circles to loosen shoulders. ● Gentle knee bends to wake up leg muscles. ● Shoulder rolls and neck stretches to improve mobility. ● A quick indoor walk or stair climb to raise your heart rate slightly. It’s also wise to check your footwear. Look for rubber soles with deep treads for better traction. Avoid smooth or worn-out shoes, and consider ice grips that attach to your boots if you live in a particularly snowy area. Winter doesn’t have to be a season of fear. By investing just 10-15 minutes a day in these simple, safe exercises, you can build the strength and confidence you need to navigate the season safely. You are giving your body the tools it needs to

Cómo las prescripciones sociales pueden mejorar la salud cardiaca
English Las enfermedades cardíacas son la causa principal de muertes de mujeres en EE.UU. La mayoría de nosotras conocemos las recomendaciones estándar: Hacer más ejercicio, comer mejor, dejar de fumar y controlar el estrés. Pero incluso con las mejores intenciones, estas instrucciones podrían sentirse abstractas, especialmente si vives en un vecindario sin un lugar seguro para caminar, si no tienes fácil acceso a productos agrícolas frescos o si pasas días sin hablar con otra persona. ¿Qué pasaría si tu proveedor de atención médica pudiese referirte a un coro comunitario, darte un vale de un mercado de productores agrícolas o decirte que te inscribas en una caminata con guía en tu parque local como si estas opciones fuesen medicamentos? Esa es la idea de las prescripciones sociales. ¿Qué son las prescripciones sociales? Las prescripciones sociales son un sistema de referencias que conectan a personas con actividades y recursos comunitarios que no son de índole médica para abordar situaciones que afectan su salud. Imagina que son como puentes entre el consultorio de tu proveedor de atención médica y los otros aspectos de tu vida. Julia Hotz, periodista y autora de The Connection Cure, el primer libro que se ha escrito de prescripciones sociales, ha dado seguimiento a este movimiento a medida que se propagó desde el Reino Unido a más de 32 países. “Las prescripciones sociales recibieron su nombre por cómo se abordan factores sociales que afectan la salud”, explicó. “Refiriéndose a que las personas sin acceso a espacios verdes, comida saludable y nexos sociales importantes experimentan más disparidades médicas”. Hotz Identifica cinco pilares de las prescripciones sociales: la actividad física, la naturaleza, el arte, el servicio y la conexión social. No es un reemplazo de medicamentos o cirugías. Pero es un suplemento poderoso, un método para tratar a una persona íntegramente y no solo abordar el diagnóstico. Los riesgos cardiacos ocultos de tu vida social Cuando la mayoría de personas piensan en el riesgo de enfermedades cardíacas, piensan en el colesterol, la presión arterial y el cigarrillo. Pero décadas de investigaciones señalan algo más profundo: Tu vida social ejerce influencia en tu salud cardiovascular en formas sorprendentes. Personas con una mala vida social tienen un 30% más de probabilidades de desarrollar cardiopatías isquémicas y accidentes cardiovasculares, según una revisión sistemática de 23 estudios. Personas adultas que rara vez o nunca recibieron apoyo social tuvieron casi el doble de riesgo de acumular tres o más factores de riesgo cardiovascular, incluyendo hipertensión, colesterol alto y diabetes, en comparación con personas con nexos sociales sólidos. Y la soledad inflige un perjuicio importante: Un estudio de 2025 determinó que personas con soledad crónica tienen un riesgo 56% mayor de accidentes cardiovasculares, incluso después de ajustar los resultados por depresión y aislamiento social”. Lee: Cómo establecer relaciones sociales si sientes soledad >> La ciencia detrás de esto es simple. El estrés, la soledad y la depresión elevan los niveles de cortisol y de marcadores inflamatorios, incrementan la presión arterial y alteran el sueño, factores de riesgo conocidos de enfermedades cardíacas. Por eso, aunque las prescripciones sociales empezaron como una respuesta a varias crisis de la salud mental, también se están reconociendo cada vez más como intervenciones cardiovasculares. De hecho, un estudio de 2025 que se publicó en Frontiers in Public Health examinó específicamente las prescripciones sociales para la salud cardiaca e identificó relaciones importantes entre prescripciones que incluían exposición a la naturaleza, actividades físicas e iniciativas para vivir saludablemente con mejores desenlaces clínicos cardiovasculares. “Es verdad que las prescripciones sociales tienen un historial de abordar cosas tales como el estrés, la soledad, la ansiedad y la depresión, pero también pueden ser útiles para la salud cardiaca porque se podrían prescribir actividades físicas y exposición a la naturaleza que se sabe que reducen el estrés de los sistemas cardiovasculares”, dijo Hotz. Hotz resalta como ejemplo a Walk with a Doc fundado por un cardiólogo de Columbus, Ohio, y que ahora tiene más de 500 sucursales en todo el mundo. “He hablado con muchas personas que han mejorado directamente su salud cardiovascular con estas caminatas”, dijo. El poder de la prescripción ¿Por qué los pacientes necesitan una prescripción para algo que podrían hacer por su propia cuenta? Expertos resaltan el “efecto oficial” de una prescripción formal. Si un proveedor de atención médica dice que una actividad social es parte de tu plan de atención, no solo es una buena idea, el paciente lo toma más seriamente y sigue las instrucciones. “Si tu doctor dice que esta es una parte importante de tu proceso de bienestar y de salud, es más probable que cumplas con eso”, dijo Adrienne Hundley, jefa de estrategia comunitaria de SocialRx, una organización sin fines de lucro que establece conexiones entre pacientes y experiencias artísticas, culturales y comunitarias. Tener una prescripción también podría disminuir la carga financiera de participar en actividades comunitarias porque pueden incluirse en planes terapéuticos formales por lo que pueden tener cobertura de seguros médicos de compañías que trabajan en conjunto con organizaciones tales como SocialRx. Además, los programas Medicaid y Medicare Advantage cada vez abordan más los factores sociales de la salud mediante iniciativas de bienestar que incluyen la cobertura de prescripciones sociales. Adicionalmente a las aseguradoras, también puede encontrarse financiamiento a través de programas de equidad médica de hospitales, subvenciones médicas públicas u organizaciones comunitarias sin fines de lucro. SocialRx cubre los costos de participación de sus miembros, ofrece programas en español y en otros idiomas y frecuentemente incluye asistencia para el transporte. Asesores de atención manejan la logística, dando seguimiento y motivación, hablando con los pacientes después de cada experiencia y ayudando a los pacientes a seguir con el tratamiento. Todo esto es útil para eliminar obstáculos que podían evitar que pacientes participen individualmente en esas actividades. El modelo de SocialRx incluye 12 dosis mensuales de experiencias comunitarias a lo largo de un año. Hundley compartió la historia de una mujer de edad avanzada que no había salido de su hogar en más de seis meses. Su asesor

Postpartum Sexuality Survey Reveals Common “Desire Gap”
Intimina study of 3,000 mothers reveals the complex reality of postpartum sexuality Giving birth is, for most women, the most significant and happiest event of their lives, marking the beginning of an extraordinary new chapter. However, to understand how women truly feel during the sensitive period, Intimina conducted an extensive survey of 3,000 women across the UK, France, and Spain who have given birth within the last 12 months. The findings show there is a significant “Desire Gap” and prove that while the body may heal, the journey back to one’s sexual self often follows a much longer, more personal timeline. The Reality of Postpartum Intimacy: 10 Key Insights The Identity Struggle The shift into motherhood often overshadows a woman’s sense of self. 24.5% of respondents feel like a “mother” first and a “sexual being” second. This feeling was most pronounced in Spain, where 27.9% of women struggled to switch between these roles. The Pressure of the Medical Milestone The “six-week green light” is often more stressful than helpful. While some found it reasonable, 17.4% of women felt pressured by this deadline, and 15.1% felt “broken” because they weren’t ready when the doctor said they could be. Intimina’s medical expert, Dr. Susanna Unsworth comments: “Postpartum recovery is often reduced to timelines, but in reality it is far more complex. The six week check is an important opportunity to assess how both mother and baby are recovering, not a signal that women should feel physically or emotionally ready to resume intimacy. Many are still navigating significant changes at this stage, including exhaustion, hormonal shifts, and a shift in identity as they adjust to motherhood.” Physical Barriers to Intimacy Returning to intimacy is often physically daunting. 34.3% of women cited extreme exhaustion as their primary barrier, while 31.4% dealt with physical discomfort like vaginal dryness, and 30.9% admitted to a literal fear of pain. The Hidden Burden of Guilt Guilt is a dominant force in the postpartum experience. 44.2% of women felt guilty for not wanting sex, while 40.7% felt guilty for prioritizing their own pleasure over the baby’s needs. France saw the highest levels of partner-related guilt at 47.5%. Honesty and “Performance” Couples often struggle to communicate about their changing sex lives. While 35.3% are completely honest, 20.9% of women admit they “perform” or fake interest to keep their partner happy. Moments of Empowerment Despite the challenges, many women find new strength in their bodies. A significant 42.2% feel a new level of respect and awe for what their body has achieved, and 31.3% report that their orgasms have actually become more intense since giving birth. A New Approach to Connection Intimacy often evolves into something deeper and more exploratory. 34.7% of women see sex now as a way of “re-learning” their body, while 32.8% say it has become less about the “act” and more about feeling seen and appreciated. The Clinical Shift Hormonal changes can make intimacy feel less natural. 49.2% of women noted that physical changes made sex feel “clinical” rather than spontaneous. This was felt most strongly in the UK, where 54.3% of women reported this shift. There is also a surprising “pleasure peak” for many. 31.3% of women reported that their orgasms have actually become more intense since giving birth. In the UK, this positive shift was reported by 32.4% of respondents. The Source of Pressure The drive to “bounce back” comes from multiple angles. 26.5% point to their partner’s expectations, while 23.2% blame the unrealistic standards set by social media influencers. The Path to Better Support Mothers know exactly what they need to thrive. 33.3% believe that more honest conversations with friends and other mothers would have changed their experience, and 37.3% noted that better access to pelvic floor therapy or intimacy products would have empowered their return to sexual health. “We hope to encourage a more open conversation around the ‘Silent Year’ of postpartum healing,” says Dunja Kokotović, Global Brand Manager for Intimina. “Our study of 3,000 women reflects a shared journey through the complexities of new motherhood. It is time to evolve past the standard six-week benchmark and prioritize a woman’s personal readiness instead. We want to empower mothers to listen to their bodies, knowing that the only ‘right’ timeline is the one that feels right for them.” “What is clear from this data is the need for a more compassionate and individualised approach to postpartum care. This includes better access to pelvic floor physiotherapy for all women, more open conversations about recovery and intimacy, and reassurance that there is no single ‘normal’ timeline when it comes to reconnecting with your body,” concludes Dr. Unsworth. *The research was conducted by Censuswide, among a sample of 3,046 Postpartum women or women who have given birth in the last year in the UK, France, and Spain. The data was collected in March and April 2026. Censuswide is a member of the Market Research Society (MRS) and the British Polling Council (BPC), and a signatory of the Global Data Quality Pledge. We adhere to the MRS Code of Conduct and ESOMAR principles. Source link

Propecia for Women: Does It Work and Is It Safe?
Who Is and Is Not a Candidate This is the most important part of the conversation, and it is why finasteride for women should always involve a thorough consultation rather than a quick prescription. Women who cannot take finasteride include anyone who is pregnant, trying to become pregnant, or not using reliable contraception. Finasteride can cause serious birth defects in male fetuses, and even skin contact with broken or crushed tablets carries a risk. This is a firm contraindication, not a preference. Premenopausal women who are prescribed finasteride off-label must be using reliable birth control and must be counseled clearly on this risk. Women who may be appropriate candidates include postmenopausal women with female pattern hair loss, premenopausal women who are not and do not intend to become pregnant and who are using reliable contraception, and women who have not responded adequately to first-line treatments like minoxidil. Even for appropriate candidates, finasteride is not the right choice for everyone. Hormonal context matters, the underlying cause of the hair loss matters, and whether other factors like thyroid function or iron levels have been addressed first matters. This is why we do not prescribe it in isolation at NHLMA. What Are the Alternatives? Whether finasteride is right for you or not, there are several other treatments with strong evidence for female pattern hair loss worth knowing about. Topical minoxidilis the most established FDA-approved treatment for women with pattern hair loss. It works differently from finasteride, stimulating follicle activity rather than addressing DHT, and it is appropriate for a much broader range of patients including premenopausal women. Low-level laser therapy (LLLT)uses specific wavelengths of light to stimulate follicle metabolism and is a well-tolerated, non-hormonal option that works well as part of a combined protocol. PRP (platelet-rich plasma)and exosome therapy both work by delivering concentrated growth signals directly to the scalp, supporting follicle health and encouraging the transition from resting to active growth phases. These are particularly effective when hair loss is in the earlier stages. Nutritional and hormonal optimization through comprehensive labs is often the missing piece. Addressing iron deficiency, thyroid dysfunction, or hormonal imbalances that are driving the hair loss in the first place can make everything else work better and sometimes resolves shedding on its own. Spironolactone is another off-label option for premenopausal women with androgen-driven hair loss, often considered before finasteride given its longer track record of use in women. What We Actually See in Practice At NHLMA, finasteride is one tool among many, and whether it belongs in a patient’s plan depends on a thorough evaluation first. We look at the type and pattern of hair loss, hormonal and nutritional labs, medical history, and reproductive considerations before discussing it as an option. For postmenopausal women with confirmed androgenetic alopecia who have not responded to first-line treatments, it can be genuinely effective. For younger women, we typically explore other options first and have a detailed conversation about the risks before considering it. What we do not do is treat female hair loss the way male hair loss is treated with a simple prescription and no deeper investigation. The two are fundamentally different problems that require different approaches. Source link


