

By Lexi Mitchell When people think about military service, they often picture discipline, strength, and resilience. What they don’t always see is the hidden cost—the physical and emotional pain that service members carry long after the mission ends. Officer training is infantry-based, and as a smaller female in a physically demanding environment, I learned firsthand how unforgiving that world can be on the body. The Army trains everyone to push beyond limits—but there’s a fine line between endurance and injury. During one combatives training session, I tore my rotator cuff. It was just one of many injuries that came from carrying heavy rucksacks, weapon systems, and gear that easily weighed over 60 pounds—sometimes for miles, over and over again. The physical strain doesn’t discriminate. It doesn’t matter your size or gender—everyone hurts. Feet blister and bleed after a 12-mile ruck march, and yet you wake up in the woods the next day and do it all over again. There’s rarely time for the body to recover before the next test of strength or endurance begins. The culture rewards pushing through pain, and for most of us, stopping wasn’t an option. But pain isn’t just physical. The constant pressure—mental, emotional, and physical—takes a toll that many don’t talk about. Under that much stress, your body’s healing process slows down. Your immune system weakens. When all three—mind, body, and spirit—are under siege, the effects can be long-lasting. Today, I live with the consequences of those years of service. What many people don’t realize is that pain isn’t always visible. I often hear comments like, “You’re young, you look healthy, you look fine.” But the truth is, my pain lies within me. It doesn’t show on my skin, but it affects every part of my life. It’s invisible—but it’s real. I share this not to complain, but to inform. As a veteran and as someone who values facts, I know that stress directly impacts the body’s ability to heal. Chronic pain isn’t weakness—it’s biology. And yet, too many veterans continue to “suck it up,” ignoring pain until it becomes unmanageable. Veterans often carry invisible wounds alongside the visible ones. Pain management isn’t just about medication—it’s about understanding the full human experience of those who served. It’s about listening, validating, and creating care systems that honor both strength and vulnerability. To my fellow veterans: you are not alone. Pain does not define your worth. Seeking help isn’t a sign of weakness—it’s a continuation of your service, because it allows you to reclaim your health and your life. Resources for Veterans in Pain Source link

How Social Prescribing Can Improve Heart Health
Español Heart disease is the number one killer of women in the U.S. Most of us know the standard advice: Exercise more, eat better, quit smoking, manage stress. But even with the best intentions, those instructions can feel abstract, especially if you live in a neighborhood without a safe place to walk, can’t easily afford fresh produce, or go days without talking to another person. What if your healthcare provider could connect you to a community choir, give you a farmers market voucher, or tell you to sign up for a guided walk through your local park and call it medicine? That’s the idea behind social prescribing. What is social prescribing? Social prescribing is a referral system that connects people to non-medical, community-based resources and activities to address the root conditions shaping their health. Think of it as a bridge between your healthcare provider’s office and the rest of life. Julia Hotz, journalist and author of The Connection Cure, the first book written on social prescribing, has followed the movement as it spread from the United Kingdom to more than 32 countries. “Social prescribing got its name from the way it intends to address the social determinants of health,” she explained. “Meaning that people without access to green space, people without access to healthy food and people without access to strong social supports would experience further health disparities.” Hotz identifies five pillars of social prescribing: movement, nature, arts, service and social connection. It’s not a replacement for medication or surgery. But it’s a powerful complement to both, a way of treating the whole person, not just the diagnosis. The hidden heart risks in your social life When most people think of heart disease risk, they think of cholesterol, blood pressure and smoking. But decades of research point to something deeper: Your social world shapes your cardiovascular health in ways that may surprise you. People with poor social health were 30% more likely to develop coronary heart disease and stroke, according to a systematic review of 23 studies. Adults who rarely or never received social support had nearly twice the risk of accumulating three or more cardiovascular risk factors — including hypertension, high cholesterol and diabetes — compared to those with strong support. And loneliness carries its own toll: A 2025 study found that people with chronic loneliness had a 56% higher risk of stroke, even after adjusting for depression and social isolation. Read: How to Make Connections When You’re Lonely >> The biology behind this is straightforward. Stress, loneliness, and depression each elevate cortisol and inflammatory markers, raise blood pressure, and disrupt sleep, all recognized risk factors for heart disease. This is why social prescribing, though it originated as a response to mental health crises, is increasingly recognized as a cardiovascular intervention too. In fact, a 2025 study published in Frontiers in Public Health specifically examined social prescriptions for heart health and found strong relationships between prescriptions involving nature exposure, physical activity and healthy living initiatives and improved cardiovascular outcomes. “It’s true that social prescribing does have a track record of addressing things like stress, loneliness, anxiety, depression, but it can also help heart health in that it could be for activities involving movement, activities involving nature, which are known to de-stress the cardiovascular systems,” Hotz said. Hotz highlights Walk with a Doc, launched by a cardiologist in Columbus, Ohio, and now operating more than 500 chapters worldwide, as a prime example. “I’ve spoken with lots of people who have directly improved their cardiovascular health through these walks,” she said. The power of the prescription Why do patients need a prescription for something they can do on their own? Experts point to the “authority effect” of a formal prescription. When a healthcare provider says a social activity is part of your care plan — not just a nice idea — patients take it more seriously and follow through. “If your doctor says this is an important piece of your health and well-being journey, you’re probably more likely to follow through on that,” said Adrienne Hundley, head of community strategy for SocialRx, a nonprofit that connects patients with arts, cultural and community-based experiences. Having a prescription may also ease the financial burden of participating in community activities by tying them to formal treatment plans so they can be covered by health insurance, which may partner with organizations like SocialRx. Additionally, Medicaid and Medicare Advantage programs increasingly address social determinants of health through wellness initiatives that include social prescription coverage. Beyond insurers, funding can also flow through hospitals’ health equity programs, public health grants, or community nonprofits. SocialRx covers participation costs for members, offers programming in Spanish and other languages, and often includes transportation assistance. Care navigators handle the logistics and serve as accountability partners, checking in after each experience and helping patients stay on track. All of this helps remove barriers that may prevent patients from engaging on their own. SocialRx’s model involves 12 monthly doses of community experience over a year. Hundley shares the story of one older woman who had been nearly housebound for over six months. Her care navigator connected her to a community choir. She went once, came back and by the third month had stepped in as a piano accompanist. By the end, she was the choir’s assistant director at the senior center multiple times a week. “I have found my people, I have found my community, and I have found a renewed lease on life,” she told the team. That kind of transformation can have a powerful physiological impact. According to SocialRx, nearly 4 out of 5 of their members with positive indicators for mental health concerns — anxiety, depression or loneliness — show improvement after their last dose as measured by the The World Health Organization-Five Well-Being Index. Given the links between these conditions and cardiovascular risk, those figures may carry implications for heart health as well. Social prescriptions require a personalized approach Social prescriptions can look wildly different from one person to

Let’s Talk About Vaginismus
Estimated reading time: 5 minutes In the first of our Let’s Talk About series on YouTube, we explore vaginismus. Vaginismus is a form of pelvic floor dysfunction that causes the pelvic floor to involuntarily contract when vaginal penetration is attempted. It can feel as though there is a wall blocking the entrance, which can strike fear into your heart as this is completely outside of your control. With between 5 and 17%1 of women being impacted by the condition, it is critical that we talk about it. In its primary form, vaginismus can prevent penetration when first using tampons or trying to insert a menstrual cup. It can also prevent penetrative sex. For this reason, primary vaginismus is generally discovered during puberty or in early adulthood. The secondary form of vaginismus can occur following childbirth, during menopause or following pelvic surgery or trauma. That trauma can be physical or chemical in nature (such as a bad fall, radiotherapy for cancer treatment or an infection). Lastly, there is a spontaneous form of the condition which can happen at any point in life. This spontaneous is the body’s natural defence mechanism if penetration is forced, but it can also occur when a tampon or vaginal weight is being used. In that instance, the pelvic floor involuntarily contracts preventing removal of the weight or tampon. This is not considered true vaginismus as it’s not a chronic condition and can generally be resolved without extended treatment. How Can You Tell if You Have Vaginismus? Many women mistakenly believe that the initial difficulties, discomfort and pain when first using tampons or trying penetrate sex is vaginismus. It is normal to have some discomfort and pain when you first attempt penetration but it typically resolves over time with practice. In the case of vaginismus, there is no progress even with repeated practice. This is highlighted in the following two graphs. The first shows how discomfort and pain are reduced under normal circumstances as penetration is practiced. Normal Response to Penetration The first shows how discomfort and pain are reduced under normal circumstances as penetration is practiced. Normal pain and discomfort with penetration (when starting out). Vaginismus Response to Penetration The second shows how, with vaginismus, there is no reduction in discomfort or pain, even with persistent practice. Vaginismus pain and discomfort with penetration (when starting out). Studies Into Vaginismus As with other forms of pelvic floor dysfunction, vaginismus isn’t widely studied, however, the studies that have been completed provide some interesting insights into the condition. We have highlighted some studies in this episode. The first revealed heightened sensitivity at rest2 in the pelvic floors of women with vaginismus. If you have read our page on pelvic floor dysfunction, you will have learned that the goal of any pelvic floor training is to return the pelvic floor to an optimal resting length. It is believed3 that the heightened sensitivity experienced by women with vaginismus results in increased pelvic floor hypertonicity. This could be an indication of more fight-or-flight activity in the nervous system. This idea is somewhat bolstered by the second study4 which scanned the brains of women with vaginismus against controls without the condition. That study founds structural changes in the part of the brain responsible for anxiety and fear in the patients with vaginismus, providing the notion that vaginismus may be a fear-related condition. In my book, I explain how the brain cannot tell the difference between what you are thinking and something that is currently happening. Worrying and fearful thoughts have a tendency to place tension into the body, and in the case of vaginismus, this could be a major contributing factor to the condition. Diagnosis and Treatments Getting properly diagnosed and having your vaginismus graded is a first step in your journey towards recovery. In the lower grades, some pelvic floor relaxation, meditation and cognitive behavioural therapy can go a long way towards overcoming the condition. It can be really beneficial to undertake therapy along with your partner as this can help with trust and bonding, which in turn can help communicate a message of safety to your nervous system. In the later grades of vaginismus, dilator therapy may be suggested as an addition to the other exercises and therapies. We’ve shared an earlier article on 5 steps to overcome vaginismus, and have created pages in our knowledge portal sharing information on the condition and it’s conservative and invasive treatments. You will find a lot of information in my book and I have just opened the discounted presale of my course on overcoming vaginismus which will be released on March 18th 2022. If you have questions, jump over to our newly launched community where you will find a space specifically for vaginismus. References Pacik PT, Geletta S. Vaginismus Treatment: Clinical Trials Follow Up 241 Patients. Sex Med. 2017 Jun;5(2):e114-e123. doi: 10.1016/j.esxm.2017.02.002. Epub 2017 Mar 28. PMID: 28363809; PMCID: PMC5440634. Frasson E, Graziottin A, Priori A, Dall’ora E, Didonè G, Garbin EL, Vicentini S, Bertolasi L. Central nervous system abnormalities in vaginismus. Clin Neurophysiol. 2009 Jan;120(1):117-22. doi: 10.1016/j.clinph.2008.10.156. Epub 2008 Dec 13. PMID: 19071060. Unal, Suheyla & Soylu, Ahmet & Yılmaz, Uğur & Karlıdağ, Rifat & Özcan, Abdulcemal & BAydinc, Can. (2002). Vaginismus:Possible role of symphatetic nervous system. 10.13140/RG.2.2.16797.41443. Atmaca M, Baykara S, Ozer O, Korkmaz S, Akaslan U, Yildirim H. Hippocampus and amygdala volumes in patients with vaginismus. World J Psychiatry. 2016 Jun 22;6(2):221-5. doi: 10.5498/wjp.v6.i2.221. PMID: 27354964; PMCID: PMC4919261. Source link
Dissecting Cellulitis and Cardiovascular Risk — Donovan Hair Clinic
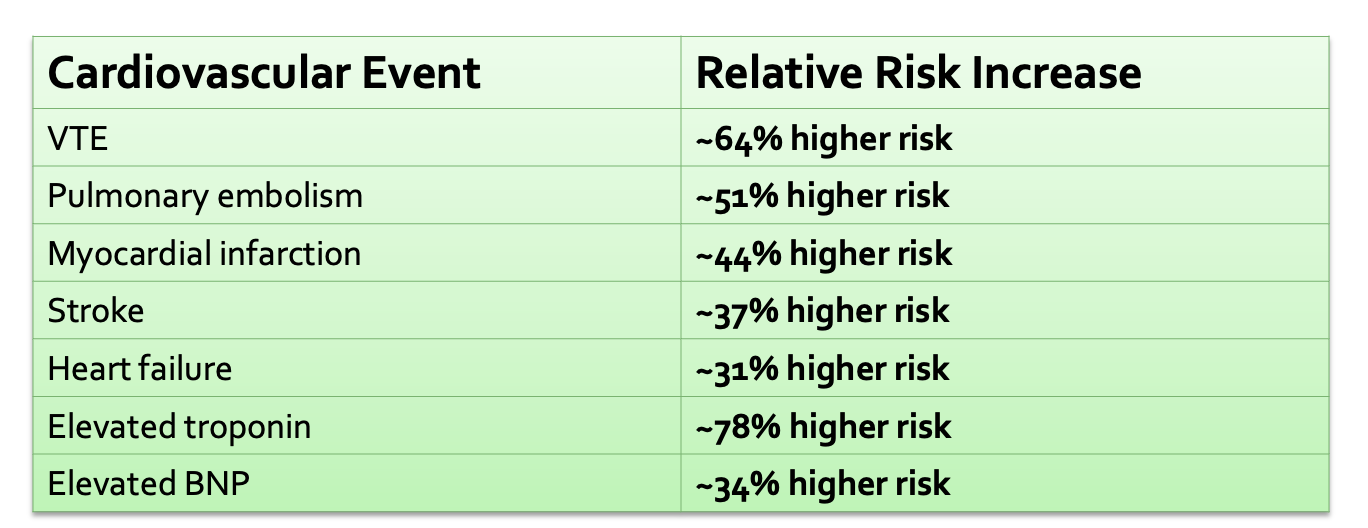
BACKGROUND & PURPOSE Dissecting cellulitis of the scalp (DCS) is a chronic, scarring inflammatory hair disease. It can be painful, disfiguring, and emotionally distressing. Similar inflammatory skin conditions such as hidradenitis suppurativa and psoriasis are linked to higher cardiovascular (CV) disease risk. The purpose of this study was to determine whether patients with DCS experience more cardiovascular problems than similar individuals without DCS. METHODS Researchers used the TriNetX global electronic-health-record database. They identified over 113,000 adults with DCS and matched them 1:1 to individuals without DCS based on age, sex, race, and key medical risk factors. They then compared how often major CV events occurred over time. RESULTS Patients with DCS had significantly higher rates of serious cardiovascular outcomes including myocardial infarction, stroke, pulmonary embolism, venous thromboembolism, atrial fibrillation, and heart failure. VTE showed the largest increased risk—about 64% higher in DCS compared to controls. Source link

Celebrating March for Migraine 2026
2026 was the fifth year of The Migraine Trust’s March for Migraine challenge, where we asked our supporters to walk, run, wheel, hop, skip or even row in one instance, 100 miles across the month of March. A total of 140 people signed up to the challenge and together they raised a fantastic £12,792 which will go towards our work to support people with migraine, fund crucial new research and campaign for change. Not only did our ‘Marchers’ raise vital funds, but they also helped to raise important awareness of migraine and the impact it can have on people’s lives. The majority of our ‘Marchers’ live with migraine themselves, many with chronic migraine, so we are particularly grateful to everyone who took on the challenge while managing migraine attacks or caring for a loved one with migraine. Two of our ‘Marchers’, Bex and Ludmilla gave their reasons as to why they participated: Source link
Mufemilast demonstrates efficacy in ulcerative colitis
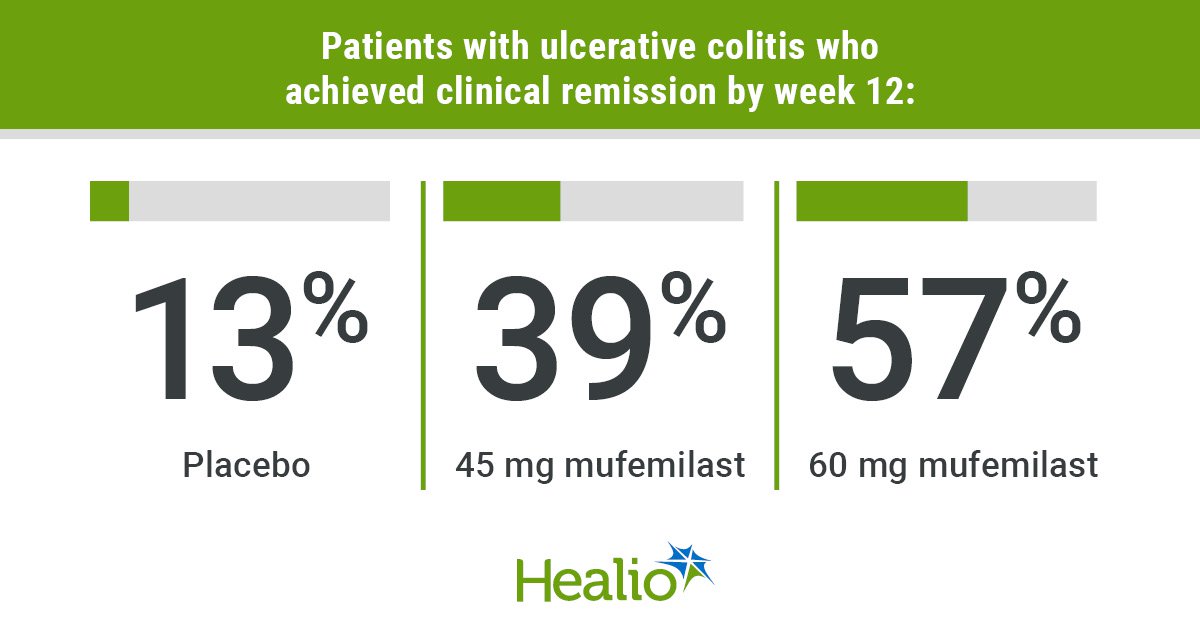
Add topic to email alerts Receive an email when new articles are posted on Please provide your email address to receive an email when new articles are posted on . “ data-action=”subscribe”> Subscribe We were unable to process your request. Please try again later. If you continue to have this issue please contact customerservice@slackinc.com. Back to Healio Key takeaways Mufemilast 60 mg improved clinical remission rate at 12 weeks, which was maintained through 24 weeks. Incidence of adverse events was similar between treatment and placebo groups. CHICAGO — An investigational small-molecule oral phosphodiesterase-4 inhibitor appeared well-tolerated and maintained clinical remission rates at 24 weeks among adults in China with ulcerative colitis, according to data presented. The novel drug, mufemilast (Hemay005, Tianjin Hemay), has been approved in China for patients with plaque psoriasis, but does not have FDA approval. Data derived from Jones CR, et al. Mufemilast (oral pde4 inhibitor) for ulcerative colitis: Open-label extension results at 24 weeks from a multicenter, randomized, double-blind, placebo-controlled parallel group induction phase II clinical trial. Presented at: Digestive Disease Week; May 2-5, 2026; Chicago. Results from a recent trial were presented at Digestive Disease Week. “When looking at this drug, there are some preclinical data that are quite interesting,” presenting author Laurent Peyrin-Biroulet, MD, PhD, head of the IBD unit at Nancy University Hospital in France, told attendees at the meeting. “On top of [an impact on] inflammation, there is also an impact on fibrosis.” Peyrin-Biroulet and colleagues investigated use of mufemilast in UC by conducting a phase 2, double-blind, placebo-controlled trial of 92 patients with moderate to severe disease. Patients needed a modified Mayo score of 4 to 9, an endoscopy score at least 2, and inadequate/failed response or intolerance to conventional therapy or biologics. Participants were randomly assigned to 45 mg mufemilast (n = 31), 60 mg mufemilast (n = 30) or placebo (n = 31) twice daily for 12 weeks, after which all groups switched to 60 mg mufemilast for an additional 12 weeks. Clinical remission rate at week 12 served as the primary endpoint. Secondary endpoints included clinical remission rate at week 24 and clinical response rate at weeks 12 and 24. Analysis included 70 patients who received 60 mg mufemilast in the open treatment period. Results showed clinical remission rates improved from 13% at 12 weeks to 75% at 24 weeks in the group originally assigned placebo, and from 39% to 62% in the group that switched from 45 mg to 60 mg. Remission rates remained steady in the group assigned 60 mg mufemilast for the entire 24-week period (57% to 52%). Researchers also reported increases in clinical response from week 12 to 24 for the groups originally assigned placebo (42% to 81%) and 45 mg mufemilast (87% to 90%), as well as in endoscopic improvement (placebo: 16% to 75%; 45 mg: 42% to 66%). The group assigned 60 mg achieved an 80% clinical response rate at 12 weeks, which dropped slightly to 72% by week 24, and also demonstrated endoscopic improvement (week 12: 67%; week 24: 64%). No significant differences were observed between responses of biologic-naive and biologic-exposed patients. Two adverse events and one severe adverse event — associated with preexisting thrombophlebitis — in the 60 mg group led to trial discontinuation. Incidence of adverse events was comparable between the treatment and placebo groups and included headache, dizziness and nausea. The incidence of headache, which ranged from 9.68% in the placebo and 45 mg groups to 10% in the 60 mg group during the 12-week treatment period, dropped to 2.86% in the open treatment period. Peyrin-Biroulet noted that tuberculosis, which is endemic in China, was an additional safety outcome in the study. “Despite having 17 TB-positive patients receiving mufemilast, no reactivation of TB was observed,” he said. “[Mufemilast] has improved efficacy, significant treatment effect and dose response — which is something that is very important,” Peyrin-Biroulet said. Published by: Sources/Disclosures Source: Jones CR, et al. Mufemilast (oral pde4 inhibitor) for ulcerative colitis: Open-label extension results at 24 weeks from a multicenter, randomized, double-blind, placebo-controlled parallel group induction phase II clinical trial. Presented at: Digestive Disease Week; May 2-5, 2026; Chicago. Disclosures: Healio was unable to confirm relevant financial disclosures at time of publication. Ask a clinical question and tap into Healio AI’s knowledge base. PubMed, enrolling/recruiting trials, guidelines Clinical Guidance, Healio CME, FDA news Healio’s exclusive daily news coverage of clinical data Learn more Add topic to email alerts Receive an email when new articles are posted on Please provide your email address to receive an email when new articles are posted on . “ data-action=”subscribe”> Subscribe We were unable to process your request. Please try again later. If you continue to have this issue please contact customerservice@slackinc.com. Back to Healio Source link
New EDS Patient: Where Do I Begin?
Did you recently get diagnosed with Ehlers-Danlos syndrome (EDS), and feel overwhelmed and confused about where to turn for help? What was described to me years ago as a rare condition is now believed to be much more prevalent, particularly when combined with the broader diagnosis of joint hypermobility disorder or hypermobility spectrum disorder (HSD). Still, many, like me, wait years to find out what is really the problem. Being diagnosed at the age of 54 with a condition I was born with lit a spark in me to do all I could to help others learn to cope. We have to wonder, if so many of us are living with the chaos and confusion of this condition, then why do we feel so lost as to where to begin to help ourselves? Shouldn’t the medical field be right there by our side with guidance? Well, as they catch up to us and learn how to help us, let’s make it our mission to pass information forward to help those around us. That may look like setting up a support group, sharing a list of medical personnel who are willing to learn and help with EDS, and paying it forward by sharing the strategies that have worked for us—including to medical providers working to learn more, as I’ve done in the past. But meanwhile, if you’ve just been diagnosed or don’t know where to start, what can you do to begin the process of trying to get on top of this condition? This Ehlers-Danlos Syndromes (EDS) and Hypermobility Spectrum Disorders (HSD) Awareness Month, I’d like to share some of what I’ve experienced and learned during my decades of living with and managing this disease. Please note that the information in this article should not be considered as professional medical advice, diagnosis, or treatment. It is for informational purposes only and represents my opinions alone, rather than the views of the U.S. Pain Foundation. These are my personal experiences and suggestions on what has helped me improve my quality of life. I share this in hopes that others living with this condition might also learn something new and improve their quality of life, too. What is Ehlers-Danlos syndrome? EDS is an inherited disorder primarily involving problems with the body’s connective tissue. There are 13 subtypes, with various levels of severity and impact. Hypermobile EDS (hEDS) is by far the most common subtype, accounting for about 9 in 10 cases. Classical EDS (cEDS) and vascular EDS (vEDS) are the next most common types, with the remaining subtypes being diagnosed much more rarely. HSD more broadly describes connective tissue disorders causing joint hypermobility and instability; some people are diagnosed with HSD when they don’t meet all of the diagnostic criteria for EDS. While this piece is largely based on my experiences with EDS, many of these insights will apply to those with HSD as well. Some people living with EDS go through life with minimal symptoms and little pain. Others are faced with a wide range of symptoms and complications. Clinical manifestations of EDS are most often joint- and skin-related and may include: Joints: Joint hypermobility (extreme flexibility) and hyperextensibility (movement beyond the joint’s normal range); loose or unstable joints that are prone to frequent dislocations and/or subluxations; joint pain. Skin: Soft, velvety skin; skin hyperextensibility (stretchiness); fragile skin that tears or bruises easily or severely; severe scarring; slow and poor wound healing. Other symptoms, which can vary by subtype, include chronic, early-onset, debilitating musculoskeletal pain; fatigue; scoliosis or neck instability; and mitral valve prolapse. Less common symptoms or complications associated with rare subtypes can include arterial, intestinal, or uterine fragility or rupture; scleral fragility; poor muscle tone; and gum disease. Due in part to the fact that the connective tissue impacted by EDS is widespread throughout the body, there are a number of associated disorders people may deal with, including postural orthostatic tachycardia syndrome (POTS) and other types of dysautonomia; mast cell activation syndrome (MCAS); Raynaud’s disease; early-onset osteoarthritis; autoimmune conditions; migraine and other headache disorders; a number of gastrointestinal disorders; gynecologic conditions; Chiari I malformation; craniocervical instability; tethered cord syndrome; and more. EDS is often misdiagnosed as fibromyalgia, osteoarthritis, rheumatoid arthritis, lupus, multiple sclerosis, myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), or Munchausen syndrome or other psychiatric disorders. To complicate matters further, it is possible to have both EDS alongside one or more of most of these disorders. How is EDS Diagnosed? While a number of providers or specialists, including general practitioners or rheumatologists, may be initially involved in identifying or suspecting EDS, a confirmed diagnosis is often obtained by a geneticist familiar with the disease, as our symptoms can vary significantly. For some types of EDS, a skin biopsy to determine the chemical makeup of the connective tissue can help to suggest the diagnosis. Genetic testing can also help identify most subtypes of EDS—but not hEDS, the most common type. Geneticists often diagnose hEDS after ruling out other types. For some, the diagnosis of EDS is based upon the patient’s clinical findings and family history. However, while family history is key in helping diagnose EDS, particularly when genetic testing can’t help, the National Institutes of Health (NIH) has found patients who were born with EDS with no family history. And due to the difficulty of receiving a diagnosis, some people are the first in their family to be diagnosed. After receiving a diagnosis of EDS, you can work with your providers to find the best ways to manage the disease. These are some of the tips I have learned. Maintaining Physical Activity When you live with chronic pain, you can get emotionally and physically worn down, and you may sometimes feel that you have no energy to exercise. But living with EDS makes it all the more important to do just that. We need to keep our muscles strong to help support our joints, and cardio workouts also help keep our bodies in the best shape possible. Consider the stationary bike,

Premenstrual Dysphoric Disorder (PMDD) Split My Sense of Self in Two
May is Mental Health Awareness Month and National Women’s Health Month. As told to Erica Rimlinger My first period divided my life into before and after. Before I started menstruating, I was a regular 14-year-old girl: skateboarding, swimming and hanging out with my friends. Then, my period came, and within a year, it felt like my personality split in half. For two weeks out of every month, I experienced all the normal teenage ups and downs. The other two weeks, I cried hysterically in my room, physically crushed under the weight of my uncontrollable sadness and rage. I didn’t feel human and couldn’t even remember what the “real me” felt or thought. Honestly, I didn’t even know which half of me was the real me. Later, when I understood my condition as premenstrual dysphoric disorder (PMDD) and met other women with the same experiences, I heard someone describe it as “being a werewolf.” That stuck with me. At 15, I genuinely believed I had turned into a monster. Long before I learned about PMDD and had language for what I was experiencing, I was told I just had PMS with underlying mental health disorders. I cycled through diagnoses: depression, anxiety, bipolar disorder and panic attacks. These explanations described some of my symptoms, but none of them fully explained what I was experiencing. I regularly saw a therapist who wasn’t a good fit and a psychiatrist who put me on birth control pills. Neither helped. Now, on top of two weeks of PMDD symptoms, I had anxiety and terrible headaches for the entire month. I didn’t feel empowered to question anything — I just went along with it until the side effects became unbearable. Rejecting the birth control pills, I was then given an antidepressant. That didn’t work either. At some point, I stopped believing anything would. I just assumed this was who I was — angry, reactive and difficult. I thought, and desperately hoped, I’d grow out of it. I didn’t. In college, the pattern continued and got significantly worse. During the bad weeks, I lay in bed with my whole body aching from depression, feeling as if someone I didn’t know hijacked my brain. The transformation was total. In that state, I was unable to think back to a time I felt human. I hid it as best I could. I told people I was sick a lot. I canceled plans, including my own birthday celebration. No one really understood, and I didn’t know how to explain it. Looking back, I was carrying the weight of trying to live a full life while hiding half of it. 2026 My moods got significantly darker. I started having suicidal thoughts. I mentioned it casually to a friend once, asking something like, “How do you deal with the suicidal thoughts from PMS?” She looked at me, shocked, and said, “PMS does not cause suicidal thoughts.” That moment stuck with me. I knew something wasn’t right. I spent the next few years seeking help and finding limited relief. I did everything I could: therapy, medication, doctors. I was surviving until I decided to get a non-hormonal IUD. Since this birth control device doesn’t use hormones to prevent pregnancy, I was assured by my doctor I’d be safe from any mood-altering side effects. She was wrong. My mood spiraled downhill rapidly and I became suicidal again. Panicked, I called the doctor’s office to get it removed immediately. Afterward my mood lifted, but I noticed my PMDD was now worse than ever. At that point, I was forced to go on short-term disability at work. During those two months, I fully committed to getting answers and improving my condition. I tried alternative therapies, including ketamine therapy. There was some temporary relief but still no real answers. Strangely, I was finally pointed in the right direction by TikTok. By 2025, I’d gone deeper with my research, and a video describing PMDD appeared on my TikTok algorithm. The missing piece fell into place: I’d never heard of PMDD and had long stopped believing the story that I had “really bad PMS.” PMS symptoms didn’t apply to me. I didn’t have mild irritability or physical discomfort — I had weeks when my safety, relationships and ability to function were completely compromised. Once I had a name for it, I went to work. I documented everything — every diagnosis, every medication and every pattern I could track. I compiled all the notes I’d taken on my moods, my eating and my sleeping habits. Armed, I presented them all to my primary care physician, who ordered a blood panel. When it returned with normal results, she essentially shrugged. I then researched specialists and sent my records to a clinic in Chicago. The doctor, who showed up late and hadn’t even opened my file, wasn’t familiar with PMDD. Shocked, I blatantly said, “This is a mood disorder described in medical literature. Shouldn’t you know about this?” As a young teenager, I would have slunk out of the office, defeated again, but at that point, I wasn’t willing to just accept that anymore. I understood that if I didn’t fight for my life, nobody would. The second gynecologist I saw was also unfamiliar with PMDD. The third finally was. She not only understood the condition, she listened, validated what I was experiencing, made the diagnosis and set me on a path toward treatment. I cried when I finally had an answer, partly from relief and partly from the grief of everything I had gone through without understanding why. I grieved the relationships that didn’t survive, the opportunities I missed and the years I spent questioning myself. Today, I no longer feel the need to hide my PMDD or view it through a lens of shame. I have a treatment plan. I have tools. And I finally understand what’s happening in my own body. PMDD is still widely misunderstood — even among medical professionals. But there are answers out there and ways
The 11 Best Porn Sites for Women in 2026
If you purchase an independently reviewed product or service through a link on our website, SheKnows may receive an affiliate commission. OK friends, when you think of porn, are you immediately turned off? Yeah, we hear that. It’s 2026, and yet it’s still not an easy task to find porn that you actually want to watch, meaning a website featuring hot, actually good porn that doesn’t overwhelmingly prioritize the male gaze or the male orgasm. Sure, you can wade through the videos to find one where female pleasure and (over-the-top-slash-faked) female orgasms are the focus — but even then, there’s the distinct feeling that because of the way she’s being filmed, there is still a man calling the shots. Let’s be honest, even if you’re watching it with a male partner, you may get the sense that the porn you’re trying to enjoy isn’t for you. And that can make it harder to lose yourself in the story or the sensations the way you’d want to. Related story A Scary Amount of Young People Are Going to Porn & Google for Sex Ed In other words: where are the porn sites that cater to the female gaze, that honor female sexuality in all its beautiful forms and that don’t objectify women in a way that will have you itching to take a shower immediately after viewing (in a bad way)? Where are the porn sites that feel current and up to date with what we want from sexual media today? There are good reasons these kinds of porn are necessary, too. Porn that honors female sexuality “allows us to actually see content that was designed for us with our pleasure in mind,” Gigi Engle, a certified sex and relationship psychotherapist and resident intimacy expert at dating app, 3Fun, tells SheKnows. “This can be pretty revolutionary as most of mainstream porn is made by men for men — which can really take us out of it because it doesn’t center things we actually want to see. Seeing lots of different female-centered sex acts, a range of bodies, and lots of pleasure can help us feel better about our bodies, our pleasure, and ourselves in general.” If that’s the kind of porn you’re itching for, fear no more, because we’ve found some legitimately great porn sites for you, the modern, self-loving woman. If you’re tired of porn that feels overwhelmingly straight and cis-male-centric, you’ll be pleasantly surprised by the following selection of sites. And while we’re at it, it’s probably the right time to treat yourself to some new sex toys to really turn up the heat (our current fave is the LELO’s new Sona 3 Cruise, FYI). Quick PSA, though: please take care and don’t browse this one at your desk, because you’ll be able to access some NSFW websites from here on out. Click with caution and when it’s time for You-time, have fun! And as Engle reminds us, support these ethical porn sites by “always, always, always pay[ing] for your porn!” A version of this story was published on April 2018. Quinn Image Credit: SheKnows Audio erotica stays a fave for erotic content, and while it’s not the same as visual porn, it is something you can get off to knowing it’s made ethically and with your tastes in mind. Quinn, for example, is particularly cool with its super user-friendly interface, cast of sensual and totally dreamy voices, and curated, inclusive playlists to hit all of your tastes. And if audio erotica is hitting all the right buttons for you, try out our favorite erotic podcasts to keep the good times going. Erika Lust Image Credit: SheKnows One site Engle recommends is Erika Lust, which she says makes “queer, female-lens centered movies that are actually really high quality.” This site is all about “cinematic, artsy porn” that has actual narratives (love!) while prioritizing representation and ethical standards. If gorgeously-shot films about sapphic sex parties and swingers’ game nights sounds up your alley, click away. Dipsea Image Credit: SheKnows OK, one more audio erotica, just for fun. Dipsea is yet another excellent example of how sexy and fun it can be to tune in and listen to some sexy voices talking about sexy things. With its clean and beautiful interface, inclusive and diverse casting, and thoughtful, consent-minded stories, you’ll love to plug in and enjoy pretty much everything in their library. PinkLabel.TV Image Credit: SheKnows Another one of Engles’ favorites, PinkLabel.TV offers a true banquet of choices for your viewing pleasure. You can browse through categories like The Feminist Porn Gaze, Art Porn, Queer Porn, and Group Sex — and that’s just a taste. “Get experimental and just browse for a while until you find something that gets you going,” Engle advises. “It can be a really fun learning experience.” Bellesa Image Credit: SheKnows Imagine if Pornhub or RedTube became way, way more unapologetically female-friendly — that, dear friends, is Bellesa. You’re welcome, and enjoy. Sssh.com Image Credit: SheKnows Billed as a “smart and sexy erotic destination for women, by women,” Sssh.com allows you to access a variety of content, from videos to reading materials, all geared toward women. You’re sure to find a medium that gets the job done. XConfessions Image Credit: SheKnows Created by feminist adult filmmaker Erika Lust, XConfessions brings very real, very sexy stories submitted by various folks to life. Yes, it’s as hot as it sounds. Literotica Image Credit: SheKnows If you’re more stimulated by words than images or you’re looking for a quieter, more stealth porn session, head over to Literotica and let your imagination run wild thanks to the enticing stories submitted there. Vivid-Ed Image Credit: SheKnows Part of Vivid Entertainment and run by sex educator and podcaster Tristan Taormino, Vivid-Ed lives up to its name with articles, movies, photos, and more to help you become your best, most empowered sexual being. Kink Image Credit: SheKnows Whether you’re already an experienced lover of kinky sex acts or are just looking to test the
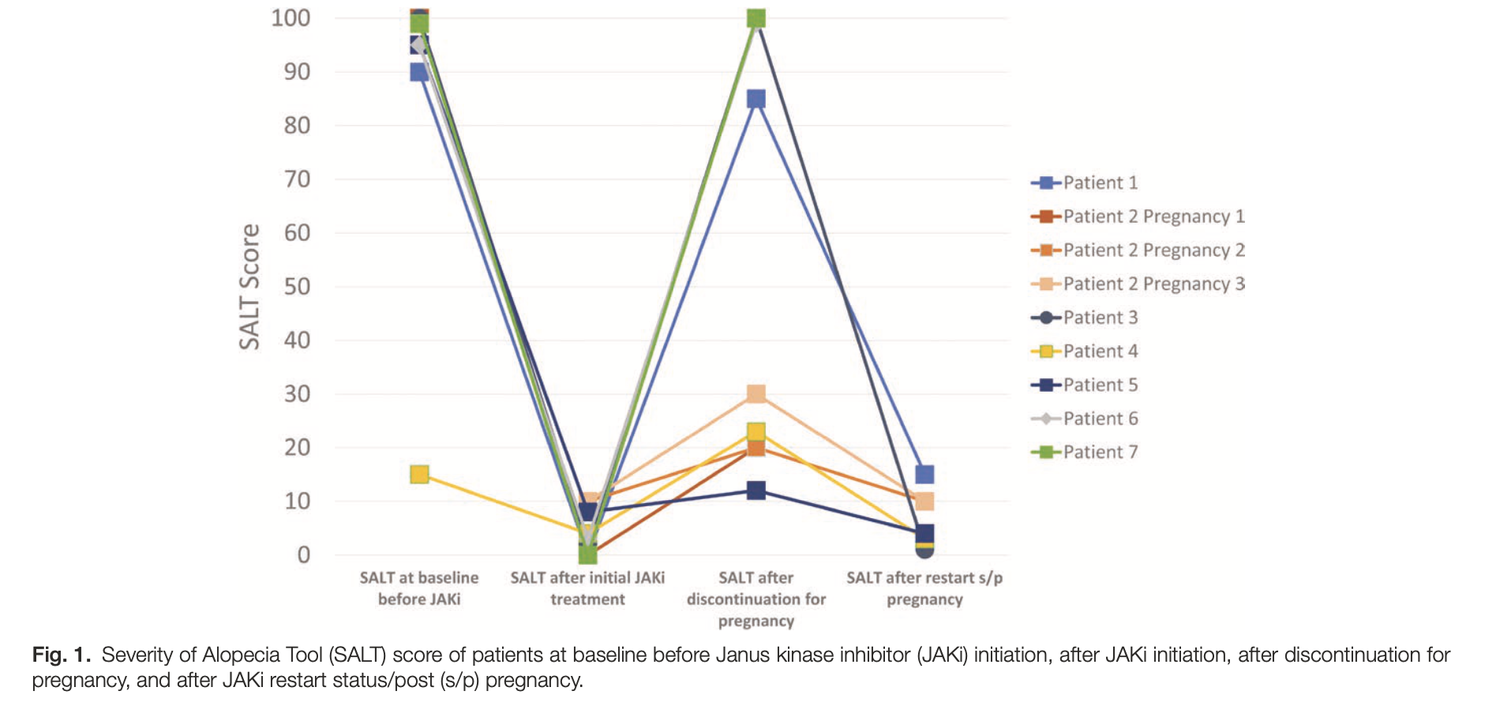
Stopping JAK Inhibitors for Pregnancy: What Happens to Hair in AA? — Donovan Hair Clinic
February 15, 2026 BACKGROUND & PURPOSEJanus kinase inhibitors (JAK inhibitors) can help severe alopecia areata (AA) regrow hair. But because safety in pregnancy isn’t fully known, and recommendations are now for women stop treatment when trying to conceive. This often leads to fear of hair loss returning. The purpose of this study was to describe what happens to scalp hair when JAK inhibitors are stopped for pregnancy — and what happens after restarting them postpartum. METHODSDoctors followed 9 women with severe AA through 14 pregnancies. All stopped oral JAK inhibitors before or early in pregnancy. Hair loss severity was measured using the SALT score before treatment, after stopping treatment, and after restarting postpartum. RESULTSEvery woman experienced significant hair loss after stopping treatment. However, once JAK inhibitors were restarted — usually within 4 months after delivery — patients regrew their hair, often back to or better than before. FIGURE 1 FROM Ogbutor C, Chen L-C, Kalil LL, et al. Discontinuation and restart of Janus kinase inhibitors due to pregnancy in alopecia areata: a case series. Int J Womens Dermatol. 2025;11:e218. used with creative commons license. CONCLUSIONSWomen with AA who must stop JAK inhibitors during pregnancy should be counseled that hair shedding is highly likely. The encouraging news is that restarting treatment after delivery (and after breastfeeding is done) led to meaningful regrowth in all cases. This study highlights the emotional burden these women face and the need for clearer pregnancy-related treatment guidelines in AA. REFERENCEOgbutor C, Chen L-C, Kalil LL, et al. Discontinuation and restart of Janus kinase inhibitors due to pregnancy in alopecia areata: a case series. Int J Womens Dermatol. 2025;11:e218. This article was written by Dr. Jeff Donovan, a Canadian and US board certified dermatologist specializing exclusively in hair loss. Source link


