

A breast self-exam is when you check your breasts, by sight and by touch, for any changes, like a new lump. And many professionals will agree that becoming familiar with what your breasts normally look and feel like is a great way in which to become aware of any changes for early concerns or cancer detection. Today, we’re going to be looking at breast lumps, what it feels like, the different types, and how to check for breast lumps aka do a breast self-exam. What Is a Breast Lump? A breast lump is a localised swelling, bump, or mass in the breast that feels different from the surrounding breast tissue, and it can vary in size, texture, and tenderness. And while it can be completely daunting, it’s important to remember that the majority of breast lumps are not breast cancer. In fact, there are many conditions that may cause benign (non-cancerous) breast lumps. On the other hand, the absence of a noticeable breast lump doesn’t mean that breast cancer cannot or hasn’t developed. This is why it’s important for women to do self-exams monthly from the age of 18, and for women over the age of 40 to go for an annual mammogram. What Does a Breast Lump Feel Like? A breast lump can feel different depending on its cause. It can be found in or around the breast tissue, or in the underarm area, and its size can vary from a pea to larger than a golf ball. Some common sensations and textures include: Firm or Hard This may feel like a solid mass within the breast Cancerous lumps are often hard and irregular Benign lumps can also feel firm Smooth and Moveable Often round or oval Can move slightly under your fingers Is often common with fibroadenomas (non-cancerous growths) Soft or Fluid-Filled May feel squishy or like a small water balloon Often tender before a menstrual period Common with breast cysts Tender or Painful Fixed in Place A lump that doesn’t move easily The Different Types of Breast Lumps For clarity, we’ll divide this up into two sections; benign and malignant. Benign means non-cancerous, and malignant means cancerous. Benign Breast Lumps Fibroadenoma: occurs primarily in women in their 20s and 30s, the lump may feel rubbery and move around freely, it’s often painless, varying in size, and can form anywhere in the breast tissue. Fibrocystic breasts: may come about in women with dense breasts, occurs naturally due to hormonal fluctuations during menstruation, may feel lumpy, swollen, and sore before a period. Breast cyst: a fluid-filled sac inside the breast that’s round or oval and may feel soft or firm. They’re smooth, moveable, can be tender, and may change in size during menstruation. Fat necrosis: scar tissue from injured breast fat that may occur after trauma, surgery, or radiation. They’re a firm, round lump, sometimes causing skim dimpling, and may mimic cancer on imaging. Lipoma: a slow-growing, fatty lump mass made of fat cells that are soft, painless, and move easily under the skin. Breast abscess: an infection (pocket of pus due to a bacterial infection) that causes a painful lump, and is often associated with breastfeeding. Symptoms include redness, swelling, and a fever. Intraductal papilloma: a small wart-like growth inside a breast, near the nipple, that can lead to nipple discharge. Malignant Breast Lumps Cancerous breast lumps are caused by abnormal, uncontrolled cell growth in breast tissue. Unlike benign lumps, they can invade surrounding tissue and spread (metastasise) to other parts of the body. Invasive ductal carcinoma (IDC): the most common type of breast cancer that begins in the milk ducts and spreads into surrounding breast tissue. Symptoms may include a hard, irregular lump, skin dimpling, and nipple inversion. Invasive lobular carcinoma (ILC): the second most common type of breast cancer that starts in the milk-producing lobules and spreads into nearby tissue. Symptoms may include thickening instead of a distinct lump, fullness or swelling, and subtle breast shape changes. Ductal Carcinoma in situ (DCIS): stage 0 breast cancer that’s abnormal cells confined to the milk ducts that haven’t invaded the surrounding tissue. Symptoms may include nipple discharge, but there is often no lump. Inflammatory breast cancer: a rare but aggressive form of breast cancer of which the cancer cells block the lymph vessels in the skin of the breast. Symptoms may include a red, swollen breast, warmth, skin that looks like an orange peel, and often without the presence of a distinct lump. Triple-negative breast cancer: hormone receptor-negative cancer, which is when there is a lack of estrogen receptors, progesterone receptors, and HER2 protein. HER2-positive breast cancer: when there are high HER2 protein levels, promoting rapid growth. Paget disease of the breast: a rare form of breast cancer affecting the nipple and often the areola. Symptoms may include red, flaky nipple skin, burning or itching, and a possible underlying lump. How To Check for Breast Lumps At-Home A simple, step-by-step guide on how to do a breast self-exam (BSE)… 1. Get in Front of a Mirror Stand undressed from the waist up in front of a mirror with your arms relaxed. Take a look at your breasts for changes in size or shape, swelling, skin dimpling (like an orange peel), redness or a rash, nipple inversion, or unusual discharge. Then, raise your arms overhead and repeat. After, place your hands on your hips pressing firmly and repeat again. 2. Lie Down Lie down and place a pillow under your right shoulder. Put your right arm behind your head. Use the pads of your three middle fingers on your left hand and choose one pattern: Circular: small circles from outer breast towards the nipple Vertical lines: up and down strips Wedge pattern: from outer breast toward the nipple and back out Use three types of pressure: light for just beneath the skin, medium for the middle tissue, and firm for the deep tissue near the ribs. Cover the entire breast, armpit area, area to the collarbone, and down
The Gut Microbiome in Alopecia Areata: Is it Really a Mainline Therapy? — Donovan Hair Clinic
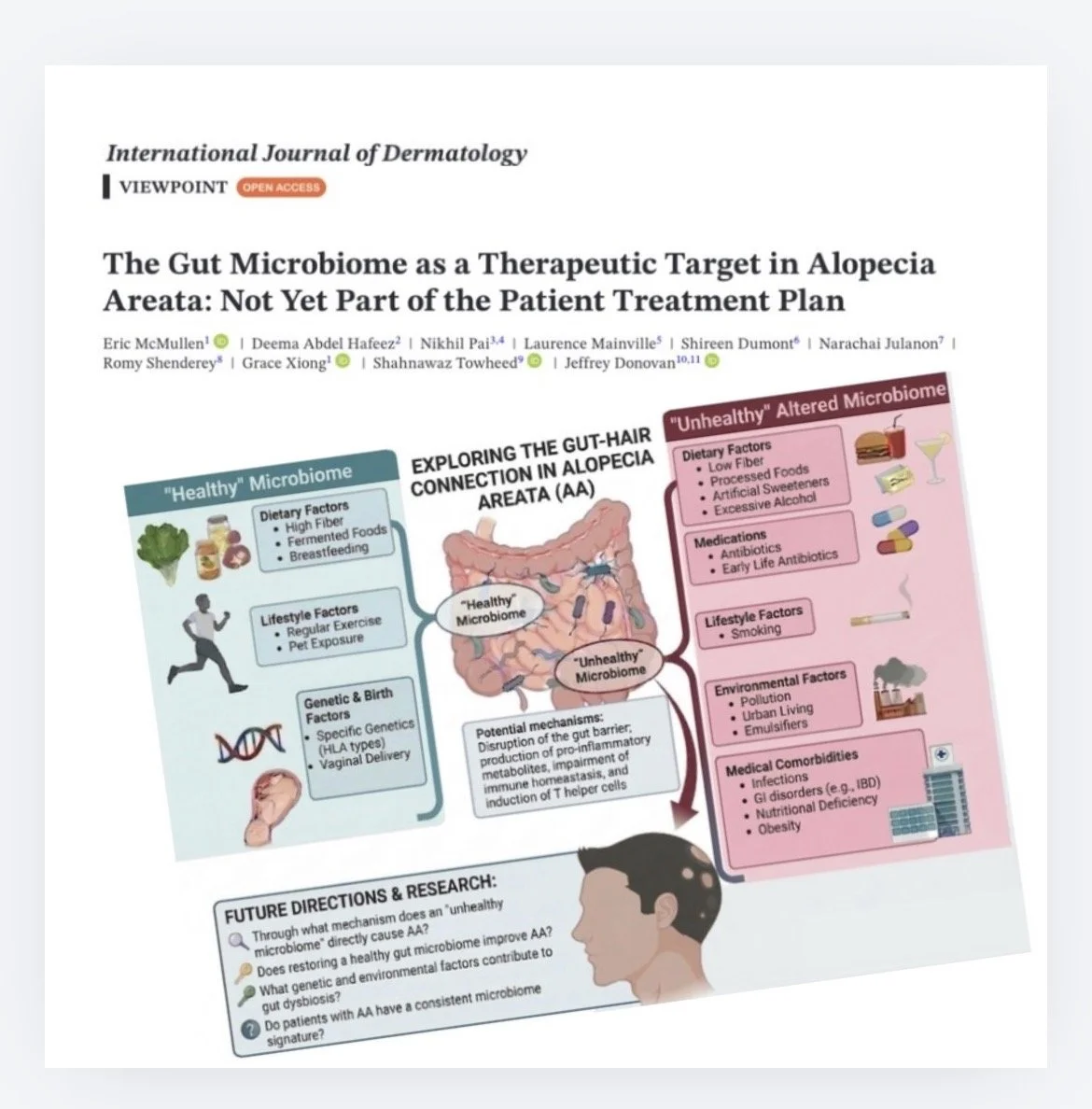
Our Microbiome Paper is Now Published It’s a great joy to share our new paper exploring the gut microbiome and whether it should currently be considered part of an evidence-based treatment plan for patients with alopecia areata. The paper is available Open Access in the International Journal of Dermatology. There has been growing interest in the “gut–skin axis” and whether gut dysbiosis may contribute to alopecia areata by influencing immune regulation, inflammation, and T-regulatory cell function. Patients are increasingly asking about probiotics, gut microbiome testing, dietary changes, and even fecal microbiota transplantation (FMT) as possible treatment strategies. Is it worth adding these evaluations and treatments? In this paper, we examined the available evidence surrounding microbiome-directed therapies in alopecia areata. While some small studies have identified potential bacterial biomarkers and very isolated reports have described hair regrowth following FMT, the overall evidence remains limited and inconsistent. A recent randomized trial of probiotics didn’t show a significant benefit. We are grateful to Wiley and the International Journal of Dermatology for publishing this Viewpoint paper. At present, the science is simply not strong enough to support routine microbiome testing or microbiome-targeted therapies as standard care for alopecia areata. Probiotics, dietary interventions, and FMT remain interesting areas of investigation—but not yet part of the evidence-based treatment plan. More rigorous longitudinal studies and stronger clinical trials are needed before these approaches can move from exciting theory to everyday clinical practice. Someday, we’ll better understand the link – and be able to better target therapies! I’ve enjoyed working with our group on this subject. Congratulations to first author Dr Eric McMullen from the University of Toronto for leading the way and for all our great discussions on this topic. And thanks to all our colleagues for their wonderful insights and hard work! Reference McMullen E, Abdel Hafeez D, Pai N, et al. The gut microbiome as a therapeutic target in alopecia areata: not yet part of the patient treatment plan. Int J Dermatol. Source link

Makary out as FDA commissioner
Add topic to email alerts Receive an email when new articles are posted on Please provide your email address to receive an email when new articles are posted on . “ data-action=”subscribe”> Subscribe We were unable to process your request. Please try again later. If you continue to have this issue please contact customerservice@slackinc.com. Back to Healio Key takeaways: Martin Makary, MD, MPH, has reportedly resigned. Inconsistency was a major component of his tenure, an expert said. Martin Makary, MD, MPH, is resigning as FDA commissioner. Politico was first to report the news on Tuesday, citing an administration official who was granted anonymity. The official told Politico that HHS Secretary Robert F. Kennedy Jr. made a decision months ago to “move on from Makary,” but the president also had to sign off. Kyle Diamantas, JD, will now lead the FDA as an acting commissioner, according to Politico. Diamantas is currently the FDA’s deputy commissioner for human foods. The FDA has not yet responded to Healio’s request to confirm the reports. Arthur L. Caplan, PhD, a professor and founding head of the division of medical ethics at NYU Grossman School of Medicine, told Healio that “it’s clear there’s a lot of dissatisfaction with [Makary], and has been for some time.” “I think the main reason for that is he’s been inconsistent at times, trying to approve drugs or speed up pathways — at other times, hindering drugs or treatments for approval,” he said. “Patient groups don’t understand what the hang up is. They’ve been pushing hard against that. One thing the FDA needs is consistency. Manufacturers want it; they need to know where the goal posts are to enable them to get across the approval line. Patients want more and more to be allowed to take risks with things that look promising. He was very inconsistent in response to that wish.” The other issue, Caplan said, is that “other things have slowed down because of cuts in personnel. That makes the biotech and pharmaceutical industries very anxious. I think Trump himself has been for some time on the side of hurrying up drug approval processes. I’m expecting that’s what we’re going to see in the next nominee to be the commissioner: speed over, if you will, caution.” Editor’s Note: This is a developing story. Please check back soon for more details. For more information: Arthur L. Caplan, PhD, can be reached at primarycare@healio.com. Sources/Disclosures Source: Healio Interviews Reference: Disclosures: Caplan reports no relevant financial disclosures. Ask a clinical question and tap into Healio AI’s knowledge base. PubMed, enrolling/recruiting trials, guidelines Clinical Guidance, Healio CME, FDA news Healio’s exclusive daily news coverage of clinical data Learn more Add topic to email alerts Receive an email when new articles are posted on Please provide your email address to receive an email when new articles are posted on . “ data-action=”subscribe”> Subscribe We were unable to process your request. Please try again later. If you continue to have this issue please contact customerservice@slackinc.com. Back to Healio Source link

The Migraine Trust urges government to incorporate migraine into the renewed Women’s Health Strategy
Migraine is a significant health issue that disproportionately affects women. Around 10 million people in the UK live with migraine and women are two to three times more likely to experience migraine than men. Migraine in women often worsens around menstruation, and has strong links to contraceptive choices, pregnancy, post-partum, and menopause. It is therefore no surprise that the lifetime prevalence of migraine is reported as 33% in women and 13% in men – before puberty, migraine frequency is the same in both sexes. Despite its prevalence and debilitating impact, it was absent from the renewed Women’s Health Strategy published earlier this week. While we welcome the government’s revival of a dedicated plan to tackle gender inequity in the health system, this is a significant missed opportunity. It is especially disappointing given that migraine sits squarely within the strategy’s four priorities. First, migraine is a condition that affects women disproportionately and often differently across the female life course. Second, it is a clear example of women’s pain being minimised or dismissed, with many women reporting that their migraine is not taken seriously, dismissed as “just hormones” or “everyday stress.” Third, it is highly suited to the strategy’s proposed shift toward earlier intervention and stronger community-based pathways – better diagnosis and treatment in primary care would prevent the condition worsening and the need for repeated appointments within secondary care. Finally, migraine has a substantial impact on work, caring responsibilities, and quality of life, making it highly relevant to the strategy’s wider goals on participation, productivity and reducing the toll of long-term conditions. Treating migraine as a priority implementation case would be a practical and credible way for government and the NHS to show that the strategy will deliver for women with common, painful, disabling but often overlooked conditions. The Migraine Trust therefore urges the government to act now to improve the migraine experience for millions of women by applying the strategy’s existing commitments to migraine care. The government can do this through: 1. Formal recognition Government and NHS England should explicitly recognise migraine as a condition that falls within the strategy’s commitment to improve care for conditions that affect women disproportionately or differently. 2. Better community pathways Integrated Care Boards should be tasked to improve migraine pathways in primary and community care, with particular attention to menstrual migraine, medication overuse, prevention, and links to reproductive health. 3. Taking women’s migraine pain seriously Implementation of the strategy’s commitments on listening to women and acting on repeated presentation should include migraine, so that women do not have to fight for a proper diagnosis or an effective care plan or review. 4. Stronger data and accountability Migraine should be included in relevant women’s health improvement metrics, including patient experience, access to appropriate treatment, and avoidable urgent or emergency care use. 5. Research across the female life course Research and innovation priorities should reflect the role of sex differences and hormones in migraine, including menstruation, pregnancy, post-partum change, and menopause. The Women’s Health Strategy was designed to improve the lives of women with common, disabling conditions that have too often been neglected. To succeed in this aim, migraine must be included in the strategy’s implementation phase. Source link

Traveling Through Your Eyes – U.S. Pain Foundation
As life moves forward, many of us have dreams of the places and things we would like to see and experience through traveling. After our four sons grew up, my husband and I planned to visit every state in the United States, and then travel the world to see other countries and experience their cultures. But then life happened for us both, and those dreams had to be set aside. At the age of 54, as my health became complicated, it was determined that I had been born with Ehlers-Danlos syndrome. This led to over 28 corrective surgeries, four years in a wheelchair, many months of recovery, and continued daily work to cope with the condition as it progresses. Then, my husband started to experience his own health challenges about four years ago, which eventually led to his diagnosis of Parkinson’s disease. So he now also lives day to day, working to maintain the best quality of life possible as he copes with his progressive condition. We had never thought about having to add medical conditions to our lives, but here we were. So those dreams we’d always had of traveling became complicated—and, eventually, just not a reality. It’s natural to mourn certain losses when you have long-term, debilitating, and painful conditions. But when life throws you those lemons, you also have to learn to live with your new situation. It is not easy to watch others participate in simple activities in life that you once took for granted, but are no longer within your reach. But you also have to decide: Will you spend the rest of your life angry, hurt, frustrated, and feeling you were cheated? Or could you find ways to adjust and accept the new life you’re now facing? When we open our eyes and look at other lives, we can see there are so many forms of loss. Yours might be a medical condition to cope with. Someone else is coping with the loss of a parent at a young age, the loss of a dear friend, or a sudden loss of a job and housing. We are not the only ones trying to find our way in life on an unexpected journey. Since our dreams of traveling were no longer a reality for us, what I decided to do is to travel through others’ eyes. This may sound silly, but when someone I am connected with tells me they are traveling somewhere, I always ask them to share photos with me and to tell me about their adventures. I want to experience the world, and this seems to be the best way I can do it safely. My sister and her husband took a trip of a lifetime recently, and I “traveled with them” to Antarctica. I joked about finding a suitcase they could sneak me into so that I could tag along, but reality meant staying at home. Still, while I wasn’t there in person, hearing their stories and seeing their photos took me on this journey, too. You might be like us and also find traveling just too difficult with the progression of your condition. But give this a try: Find fun with the travels of a friend or family member, and allow yourself to dream you were there as you see the world through their eyes. Try to make the lemon into lemonade, as the old saying goes. Show others that despite your challenges in life, you can live, breathe, and travel in your own way! This may be one way to help you be identified not by your condition, but instead as you—the person you are. May life be kind to you… —by Ellen Lenox Smith Source link

La conexión entre la menopausia y el VIH
Mujeres de todas las edades pueden contagiarse del VIH, incluyendo las de más de 50 años 1 de cada 4 personas que viven con VIH en Estados Unidos es mujer Más de 1 de cada 2 diagnósticos nuevos de VIH son para personas de más de 50 años Las mujeres mayores tienen más posibilidades que mujeres más jóvenes de recibir un diagnóstico de esta enfermedad en etapas posteriores , posiblemente porque no saben que tienen riesgo Recibir el diagnóstico en etapas posteriores incrementa el riesgo de enfermedades relacionadas con el VIH y de morir por este trastorno ¿Qué efecto tiene la menopausia en el riesgo del VIH? Las mujeres de más de 50 años siguen teniendo relaciones sexuales En un estudio reciente, 1 de cada 2 personas de más de 50 años reportó haber tenido relaciones sexuales la semana anterior. Puesto que el embarazo ya no es una preocupación para mujeres posmenopáusicas, ellas podrían no pensar en tener relaciones sexuales con protección o en hablar de eso con sus parejas o proveedores médicos. Esto significa que las mujeres podrían ser menos propensas a usar preservativos para protegerse del VIH y de otras infecciones de transmisión sexual después de la menopausia. Pero las mujeres en la perimenopausia y posmenopausia podrían tener más riesgo de infectarse con el VIH. Los cambios hormonales pueden hacer que la vagina se haga más estrecha y seca, lo cual hace que el tejido vaginal sea propenso a desgarres, y eso incrementa el riesgo de que el VIH ingrese al cuerpo durante relaciones sexuales. Algunas mujeres mayores (y sus proveedores de atención médica) atribuyen cambios de la salud a la menopausia cuando podrían causarlos algo más. Por ejemplo, los sudores nocturnos son un síntoma clásico de la menopausia, pero también son comunes para personas con VIH. La prevención del VIH durante la menopausia y años posteriores Ninguna edad es demasiado avanzada para protegerte del VIH. Empieza con estos pasos proactivos: Usa preservativos si no sabes si tu pareja tiene VIH o no Hazte pruebas de detección del VIH Habla con tu proveedor de atención médica acerca de PPrE (profilaxis previa a la exposición) , medicamento que puede prevenir el VIH. Este recurso educativo se preparó con el apoyo de Merck. Source link

Understanding Breast Cancer: What You Need to Know
Breast cancer is one of the most common cancers among women, and knowing the facts can make a huge difference. In this post, we’ll explore the early signs, the importance of mammograms, advances in treatment, lifestyle changes that can reduce your risk, emotional support options, and how you can get involved during Breast Cancer Awareness Month. What Are the Early Signs and Symptoms of Breast Cancer? Catching breast cancer early is key to successful treatment. Some of the most common early signs include finding a lump in the breast or underarm. While not all lumps are cancerous, it’s crucial to have any unusual lump checked by a healthcare professional. Another sign is noticeable changes in breast size or shape. If one breast suddenly feels or looks different from the other, it’s important to take note. Nipple changes, such as inversion (where the nipple turns inward), unexpected discharge, or discomfort in the nipple area, may also signal an issue. Additionally, keep an eye out for changes in the skin on your breasts, such as dimpling, redness, or peeling. While breast cancer typically isn’t painful in the early stages, any persistent pain should also be brought to your doctor’s attention. Getting familiar with how your breasts usually look and feel and performing regular self-exams can help you notice any unusual changes early on. How Often Should Women Get Mammograms, and Why Are They Important? Mammograms are a critical tool for detecting breast cancer in its early stages, often before any symptoms arise. Most women should start getting annual mammograms at age 40. After age 55, women may choose to switch to mammograms every two years, depending on personal risk factors and discussions with their doctor. The reason mammograms are so important is that they can detect cancer when it’s most treatable, giving women more options and a better chance at recovery. Scheduling a mammogram is simple at our practice, and you can learn more about the process here: https://adriaticawomenshealth.com/services/mammography/. What’s New in Breast Cancer Treatment? Breast cancer treatments have come a long way, with new advancements making treatments more effective and personalized. One of the most exciting developments is targeted therapy, which focuses on attacking cancer cells while leaving healthy cells alone. Immunotherapy is another promising area, as it helps boost the immune system’s ability to recognize and fight cancer cells, especially in more aggressive forms of breast cancer like triple-negative breast cancer. Personalized medicine is also making a huge impact, as doctors can now tailor treatments to the specific makeup of an individual’s cancer, improving outcomes. Proton therapy, a newer form of radiation therapy, allows for more precise targeting of cancerous tissue, minimizing damage to surrounding healthy areas. These advancements are helping patients receive more effective treatments while reducing side effects. What Lifestyle Changes Can Lower the Risk of Developing Breast Cancer? While genetic factors are important, lifestyle choices also play a significant role in reducing breast cancer risk. Staying active is one of the best ways to lower your risk. Experts recommend aiming for at least 150 minutes of exercise each week. Maintaining a healthy weight is also crucial, particularly after menopause, as excess body fat can increase the risk of breast cancer. Limiting alcohol intake is another smart move, as even moderate drinking has been linked to a higher risk of breast cancer. Quitting smoking can reduce the risk of various cancers, including breast cancer, and is always a good health choice. For those who can, breastfeeding has been shown to lower the risk of breast cancer as well. Finally, if you’re considering hormone replacement therapy (HRT), discuss the risks and benefits with your doctor, as long-term use has been associated with an increased risk of breast cancer. By adopting these healthy lifestyle changes, women can take proactive steps toward lowering their breast cancer risk. What Emotional and Psychological Support Is Available for Breast Cancer Patients? Receiving a breast cancer diagnosis can be emotionally overwhelming, but there are many resources available to help. Counseling with a mental health professional can be incredibly beneficial, offering patients a safe space to talk about their feelings and learn coping strategies. Support groups, whether in person or online, allow patients to connect with others going through similar experiences, providing a sense of community and understanding. Additionally, mind-body practices like yoga, meditation, and mindfulness can help manage the stress and anxiety that often accompany a cancer diagnosis. Many cancer centers also offer patient navigators who can guide patients through treatment, helping to connect them with emotional and psychological support services. Emotional care is a vital part of the overall treatment process, and seeking help can improve both mental and physical well-being. How Can We Support Breast Cancer Awareness Month and the Women Impacted by This Disease? October is Breast Cancer Awareness Month, and there are plenty of ways to get involved and support those affected by breast cancer. One of the simplest ways to participate is by spreading awareness. Share information about the importance of early detection, mammograms, and healthy lifestyle choices with your friends, family, and social media networks. Participating in or donating to fundraising events, like charity walks or runs, is another great way to help raise money for breast cancer research and patient support services. Wearing pink during October is a small but meaningful gesture to show solidarity with those affected by breast cancer and to raise awareness in your community. On a more personal level, if you know someone going through breast cancer treatment, offering practical help, like running errands, cooking meals, or just being there to listen, can make a big difference in their day-to-day life. Finally, encourage the women in your life to schedule regular mammograms and stay informed about breast cancer prevention. By staying informed and taking action, we can all make a difference in the fight against breast cancer. Let’s work together to raise awareness, support those going through treatment, and push toward a future where breast cancer is a thing of the past.
Lipedematous Alopecia: Topical and Intralesional Steroids Still First Line — Donovan Hair Clinic
Lipedematous scalp is a rare cutaneous condition characterized by a boggy, thick, and spongy consistency of the scalp due to thickening of the subcutaneous adipose tissue. In these conditions, the overlying skin usually appears normal, though patients often report symptoms of pain, paresthesia, or a localized “pressure” sensation. When this structural thickening is accompanied by hair loss—the condition is termed lipedematous alopecia. The exact pathogenesis remains unclear, but it is hypothesized that the expanded fat layer may mechanically compress hair follicles or disrupt the dermal microenvironment necessary for healthy hair growth. Our New Study of Lipedematous Alopecia Highlights Areas of Treatment Success Our research team performed a systematic review of this challenging condition. We uncovered 33 patients in 23 studies. There were 19 patients with with lipedematous alopecia and 14 with lipedematous scalp. These studies highlight the limited but evolving treatment landscape. Most diagnoses relied on scalp biopsy. This study was led by the great work of the first author, Katya Peri, from McGill University medical school. Topical and intralesional steroids were among the most effective treatments for lipedematous alopecia, leading to complete responses in about 50 % of patients. The most effective systemic therapies were mycophenolate mofetil with more limited data for other treatments such as hydroxychloroquine and doxycycline. The full study is published in the International Journal of Dermatology. I congratulate all of our coauthors for their efforts to better understand this fascinating and very much underrecognized condition. Reference Peri K et al. Int J Dermatol 2026 Source link
An LLM powered day in the GI clinic and endoscopy suite
by Dr Yuri Gorelik (Frontline Gastroenterology Global Taskforce 2025-6) Since the introduction of ChatGPT 3.5 in November 2022, artificial intelligence (AI) and specifically large language models (LLMs) have been set to revolutionize our daily and work life. Multiple LLM based GI utilities have been developed and researched. In this blog post I will try to provide a mini review in the form of a description of a GI practitioner workday powered by such LLM based utilities and products. Many of the specific LLM applications and use-cases I mention below are discussed in Frontline Gastroenterology’s narrative review of generative AI in colorectal practice (Frontline Gastroenterology, 2025). Morning Clinic Upon arrival at the clinic all previous follow-ups and clinic referrals for the clinic patients on your list are already summarized by one of the multiple published tools for such tasks. Soon after, the patients start to come in, all history taking and patient communication is scribed by an LLM such as the Google health medical speech to text tools (Google cloud). This text is also transformed into a structured text with clinical terms and specific disease-centered classifications. In IBD, multiple sources of medical data (notes, endoscopy, imaging) contain abundant unstructured information and such tools showed high accuracy in the identification and structuring of these texts. The need for natural language processing of IBD patient data was previously highlighted in Frontline Gastroenterology’s review on AI in IBD (Frontline Gastroenterology, 2022). Finally, each clinic comes down to patient recommendations and these are derived with the assistance of multiple LLM based decision support tools that provide recommendations based on the summary of the structured visit in the context of the relevant guidelines. Such tools can be extremely useful across multiple fields of GI, often where guidelines are inconsistent or complex and where clinicians must integrate multiple data sources with the current patient’s clinical data. Even common clinic complaints such as functional dyspepsia require integrating multiple symptoms and clinical data for optimal work-up and treatment, as described in a recent Frontline Gastroenterology guidance (Frontline Gastroenterology, 2025). Care is extended as the patients leaves with a link to chatbots that can answer questions specific to his condition. Afternoon in the Endoscopy Suite On to the endoscopy suite. Your list allows open access endoscopy received from multiple referral sites. These referrals should be evaluated to decide on appropriate settings, medication management, and type of preparation. At your location the referrals are managed by an LLM based tool which already analyzed the referrals and identified the requested procedures, the indications, pre procedural medication management (anti-coagulants, GLP-1 receptor agonists, etc.) and type of bowel preparation. Patients who come in for a procedure are well informed since a chatbot already addressed multiple concerns and questions they had regarding their upcoming colonoscopy. Just like at the clinic, during colonoscopy, you narrate findings, while an AI tool transcribes the report with high accuracy, and as clinic notes these reports will include LLM generated, guidelines-based recommendations. The patient will get an automatically generated concise letter explaining the findings and forward recommendations. Of course, the entire endoscopy is AI powered with various pathology detection and diagnosis tools, but this is a subject for a different post. Prior to heading home, you can deidentify your clinic notes and endoscopy reports from the day to a research AI agent, which is provided by all large models to look up or summarize any patient specific evidence that was not covered in guidelines or large reviews and evaluate some additional possibilities for patients. Guideline preparation in gastroenterology was already shown to benefit from augmentation with LLM-powered systematic reviews (using deep research AI tools such as those provided by all the major LLMs). If you are in a hurry, you can convert the findings to an audio podcast, using tools such as NoteBookLLM, to listen to on your way home. In summary, AI and specifically LLMs are set to revolutionize and potentially improve every aspect of our daily work as gastroenterologists, and the possibilities keep expanding. Worth mentioning that LLMs can also enable us to perform research by providing statistical and epidemiological advice and implementation and empower us to create our own tools with models that can automatically convert your prompts to apps (see vibe coding). Now briefly go over the daily description above and consider “is a human gastroenterologist really needed here and where?”, and if you are thinking “clearly in the endoscopy part” then robotics also has some surprises coming. (Visited 227 times, 1 visits today) Source link

Long-Term Disability and Chronic Pain: What the Claims Process Often Misses
By Jennifer Hess and Samantha Wladich, Riemer Hess LLC Living with chronic pain usually means adapting—again and again. People adjust schedules, modify tasks, try new treatments, and push through symptoms over and over. Many continue working not because they are well, but because they are trying to hold things together. When work finally becomes unsustainable, the long-term disability (LTD) process can feel confusing and discouraging. Pain conditions are frequently misunderstood in insurance reviews, and the way claims are evaluated often fails to reflect what daily life with chronic pain actually looks like. This article offers a general, educational look at how long-term disability claims are commonly evaluated for people living with chronic pain—and why those claims can be so difficult. Important note: This article is for general educational purposes only. It is not legal advice and is not a substitute for guidance specific to an individual’s situation or insurance policy. Hear more from these experienced attorneys during a FREE webinar, “Preparing for Your Long-Term Disability Claim,” at 1 p.m. ET on Tuesday, March 10. Register today. Why Chronic Pain Disability Claims Are So Often Challenged One of the biggest problems in pain-related disability claims is that pain often does not behave the way insurers expect disability to behave. Chronic pain can: fluctuate worsen with activity improve briefly and then return limit endurance, not just strength Insurance reviews, however, often look for steady decline, clear-cut test results, or visible impairment. When those markers are missing or unclear, insurers may conclude—incorrectly—that someone is still able to work. This disconnect is one reason long-term disability claims involving chronic pain often face higher scrutiny. A Common Scenario: When Working Through Pain Stops Working Consider this example, which reflects a pattern many people with pain will recognize. A professional living with chronic spinal pain continues working while undergoing physical therapy, medication changes, and injections. At first, they shorten their workday and recover at night. Over time, therapy triggers flares instead of relief. Medication causes brain fog. Recovery stretches into the next day. Sleep deteriorates. From the outside, it looks like they are still “functioning.” On paper, treatment is ongoing. But behind the scenes, the effort required to work becomes unsustainable. When work finally stops, insurers often ask:Why now?Why stop work if treatment was ongoing? Without context, the timing can be misunderstood. Function Matters More Than Diagnosis in Long-Term Disability Claims In most long-term disability claims, the diagnosis itself is not the deciding factor. Insurers focus instead on function. For people living with chronic pain, that usually means questions like: How long can you sit, stand, or walk? How often do symptoms flare? What happens after physical or cognitive exertion? How much recovery time is needed? Can this be repeated day after day? Someone may be able to complete tasks in short bursts and still be unable to meet the demands of regular, full-time work. Disability evaluations do not always capture that distinction unless it is clearly documented. Why ‘Trying Harder’ Isn’t the Same as Capacity A recurring theme in pain-related claims is the assumption that effort equals ability. In reality, chronic pain often limits: duration frequency consistency recovery People may push through pain at work for many reasons—financial pressure, professional identity, fear of losing benefits. That effort can later be misread as proof that work was sustainable. Understanding the difference between what can be done briefly and what can be done reliably is central to understanding disability in chronic pain-related cases. Variability Is Normal in Chronic Pain — Not a Red Flag Many people with chronic pain have good days and bad days. That variability is often used against them. Insurance reviewers may interpret fluctuating symptoms as: inconsistency exaggeration improvement In reality, variability is often one of the defining features of chronic pain. Short periods of relief do not mean the condition has resolved, especially when those periods are followed by flares or prolonged recovery. Clear explanation of symptom patterns over time helps prevent this misunderstanding. Why Baseline Function Matters When Disability Follows Treatment For many people, disability does not begin at diagnosis, or at the onset of undiagnosed symptoms or pain. It begins later—after months or years of treatment attempts and symptom progression. A baseline helps show: what functioning looked like earlier how endurance declined how treatment affected symptoms over time This matters because insurers often assume that treatment leads to improvement. When work ends after treatment begins, baseline documentation helps explain that disability developed despite care, not because care was avoided. Objective Evidence and Chronic Pain: What Insurers Look For In the disability context, “objective evidence” generally means information beyond self-report alone, such as: imaging exam findings functional testing documented observations by providers This does not mean pain must show up clearly on a scan to be real. Many pain conditions do not lend themselves to definitive test results. Still, insurers often weigh claims more heavily when some objective support exists—especially when policies scrutinize conditions labeled as “subjective,” which is often the case for pain-related diagnoses. Objective evidence is most effective when paired with clinical explanation and functional context. Treatment Does Not Always Mean Recovery Many people living with chronic pain are deeply engaged in treatment long before disability becomes an issue. Insurers sometimes interpret continued treatment as proof that improvement should follow. In reality, chronic pain treatment often focuses on: management symptom reduction preventing decline Ongoing treatment does not guarantee restored work capacity. Modifying or stopping treatment can also be medically appropriate, particularly when side effects outweigh benefits or progress plateaus. The Question Disability Claims Are Really Asking: Sustainability Whether a policy applies an “own occupation” or “any occupation” standard, the real question is the same: Can this person work reliably and sustainably over time? For people living with chronic pain, the answer often hinges on endurance, recovery, and consistency—not whether isolated tasks are possible. Final Thoughts Long-term disability claims involving chronic pain are often difficult—not because pain is unclear or insignificant, but because the claims process does not easily account for


