By Kari McBride “So, when are you going back to work?” I have danced around this question so many times that I think my dance moves now wear a permanent path. It wasn’t that I didn’t want to answer the question; it was that I didn’t know how. I felt embarrassed, guilty, and a little ashamed that I wasn’t working yet. After all, isn’t our value as a person supposed to come from what we do for a living? At least that’s how it often feels in society today. Even after four-and-a-half years of brain injury recovery, new autoimmune diagnoses, one close brush with death, daily chronic pain, and a fight for “normalcy,” I still can’t answer this question. But what I can answer is this: “When am I going to live my life?” And that answer is: Now. I am living my life now. It may be true that I was living this life yesterday, and the day before, and the year before, and so on. But I would argue that it was not the same life. I am not the same person today that I was yesterday. And I am certainly not the same person I was before my injury. My life seems to have been divided into different series: “Before the accident,” and “After the accident.” I can’t say that one is better than the other. The “before” series ends with me as a single mother, newly graduated with a Master of Social Work, employed as a school social worker, and full of energy for all that life had in store. The irony is that the “after” series starts the very next day, but features this girl I don’t recognize. She is living in my body, in my house, with my child. She is no longer working, but instead is on extended medical leave. Her new graduate degree lies off to the side, just another piece of paper. Her days are filled with therapy, appointments, medication, and pain. She is living a life I no longer recognize as my own. “So…when are you going back to work?” Am I going back? What does it even mean to go back? Life didn’t stop just because I was injured. In fact, it’s quite the opposite. In many ways, life seems to have sped up and rushed past, leaving behind only a blur. The job I had at the time is long gone, posted and filled within a few months. My child is four years older and no longer in elementary school. And that fresh degree is covered in as much dust as its accompanying textbooks. Yet somehow, I moved forward without going back. I recently found myself sitting downtown at the state capitol, waiting to meet with my state representative. My stomach was full of knots, and my palms were sweaty. I could feel the early warning signs of a migraine attack and the little daggers piercing my forehead. I had chosen my highland cow tote bag for good luck, and I kept checking to make sure my notes were safely tucked inside. This meeting was important, and nothing could shake my confidence. It had taken years of lived experience, pain, and hard work to find my own value. The moment was now, and I was ready. It was on the car ride home that I realized I may not have gone back to work, but I was working. Just in a different way. I am working to be a bold voice when so many are already talking. I am working in a way that brings meaning to my life. I am working in a way that my body and my brain allow. As it turns out, my social work degree has proved far more valuable in my journey as a patient. I experienced first-hand the value of advocacy, the impact of disability, and the stigma of chronic illness. I fought for my own self-worth and refused to let employment determine my value to society. I am living my life the way I want … the way I can. So perhaps the question isn’t “When are you going back to work?” but rather: “How are you living your life now?” —by Kari McBride Source link
Gut Microbiome and Colorectal Cancer
Nicole Pajer Nicole Pajer is a freelance writer published in The New York Times, Parade, AARP, Woman’s Day, Men’s Journal and beyond. When she’s not writing, she’s checking exotic travel destinations off her bucket list, attempting to wear out her 71-pound Doberman’s boundless energy and teaching people how to properly pronounce her last name (“It’s Pager, just like the beeper!”). Keep up with her adventures on Twitter @NicolePajer. Medically reviewed by Cynthia Sears, M.D. Source link

Are Hypopressives Beneficial for Pelvic Floor Dysfunction?
Estimated reading time: 8 minutes In this article, we will as the question Are hypopressives beneficial for pelvic floor dysfunction? If you are suffering from pelvic floor dysfunction, you may well have heard of Hypopressives; a breathing technique that uses a stomach vacuum to tap into the relationship between the pelvic floor, core and breathing diaphragm. These stomach vacuums are the same as those practiced by yogis for millennia and utilized by bodybuilders since the seventies to enhance breathing, reduce waist size and improve aesthetics. The idea that these stomach vacuums could be beneficial for treating pelvic floor dysfunctions was first suggested in the eighties when Belgian physiotherapist Marcel Caufriez began using hypopressive exercises to improve pelvic floor control in patients. With 1 in 3 women1 suffering pelvic floor dysfunction during her lifetime, finding conservative and easy to follow exercises to improve symptoms and quality of life is critical. So, let’s first explore the exercise before delving into its perceived benefits for those with pelvic floor dysfunction. How to Perform a Hypopressive Exercise (Stomach Vacuum) The hypopressive manoeuvre (also known as an apnea) involves emptying the lungs completely and immediately closing the airways to prevent air reentering the lungs. Following this, the abdominals are relaxed and the ribcage is expanded which creates a stomach vacuum causing the abdominals the be drawn upwards and inwards. The vacuum can also be seen on the back of the body and around the shoulder blades. Follow the steps below to perform the hypopressive manoeuvre which is shown in the animation. Steps to Perform a Hypopressive Apnea Perform three breath cycles where you inhale and exhale. On the third exhalation, empty the lungs fully, this will include contraction of the abs to empty the reserve volume from the lungs. Close your airways to prevent air from reentering the lungs. Take your apnea. To do so, relax the abdominals and expand the ribcage out to the sides in the same motion used when breathing but without taking air in. Hold for a count of 4. Relax the ribcage and abdominals before taking your next inhalation. Animation of a Hyperpressives stomach vacuum Should You Replace Kegels With Hypopressives? For those suffering from a Pelvic Organ Prolapse, the uplifting motion produced when performing an apnea can feel quite relieving on the prolapse, as is my experience with my own rectocele. Of course, feeling some immediate relief doesn’t necessarily mean that there are proven benefits. Marketing of hypopressive training is strong, and some campaigns even suggest using hypopressives as an alternative to Kegel exercises (Traditional Pelvic floor muscle training). In keeping with the usual approach on this website, we will explore the research to see if this makes sense, and to discover the proven benefits of practicing hypopressives. Traditional pelvic floor muscle training (Kegels) as a treatment for incontinence and prolapse is backed by decades of research confirming the benefits. Hypopressives, on the other hand, have only been studied during the last decade. The first study2 into hypopressives compared a group performing Kegels with another performing hypopressives. The conclusion was that hypopressives were less effective than Kegels alone. A subsequent study3 in 2012 had three groups; one performing hypopressives plus Kegels, a second performing Kegels alone and a control group. That study found that both groups performing exercises did better than controls, however; adding hypopressives to Kegels didn’t improve pelvic floor function and those who practiced only Kegels had superior pelvic floor endurance. Another 2012 study4 directly compared a group performing Kegels with another performing hypopressives and found that both groups showed similar improvements. Since those early studies, there have been numerous other studies, none of which have confirmed that you should ditch your pelvic floor exercises in favour of a hypopressive practice, however; through the course of these studies, the true benefit of hypopressives has been revealed. Seated Hypopressive Pose showing the apnea. A Program of Hypopressive Exercises Showed Positive Results in Post-partum Abdominal Diastasis5 The Real Benefits of Hypopressive Exercise If you are suffering from pelvic floor dysfunction, it is very likely that you also have some core weakness. This is where hypopressives can provide benefits. Whereas the early studies into hypopressives did not substantiate the suggestion that they should be used as an alternative to Kegels, they did reveal improvements in the strength of the transverse abdominis (TrA), one of the key core muscles. A 2021 study6 exploring how the abdominal muscles change during hypopressives found that hypopresives significantly increase the thickness of the TrA and internal oblique during the exercise in comparison with the muscles at rest. With that said, you should’t rush to swap your core exercises with hypopressives. A 2020 study7 that looked at the pelvic floor and abdominal muscle response during hypopressives did note that the muscles showed increased activation during the exercises, but not sufficiently to create strength gains. They did, however, suggest it could have an endurance effect. Further studies would be needed to substantiate that hypothesis. Why Practice Hypopressives? So why bother practicing hypopressives if they aren’t going to heal your prolapse or cure your incontinence? I have three reasons why I personally practice hypopressives, and why I included them in some of the breathing modules of my Eight-phase training course. Reason 1 One of the main reasons I like to practice hypopressives is because it relieves the symptoms of my rectocele. I generally only feel symptomatic if I allow myself to get constipated and have to strain to poop. When I get the heavy dragging feeling of the prolapse, I practice my hypopressives and it helps to reduce the symptoms. I also find inversions to be helpful with symptom relief. Reason 2 One of the triggers for the symptoms of prolapse, which is also a cause of leakage during stress incontinence, is increased intraabdominal pressure. When you practice hypopressives, you tap into the relationship between the breathing diaphragm, the core and the pelvic floor. I find that my hypopressive practice helps me to feel and manage this
FAPD and Discordant Anisotrichosis — Donovan Hair Clinic
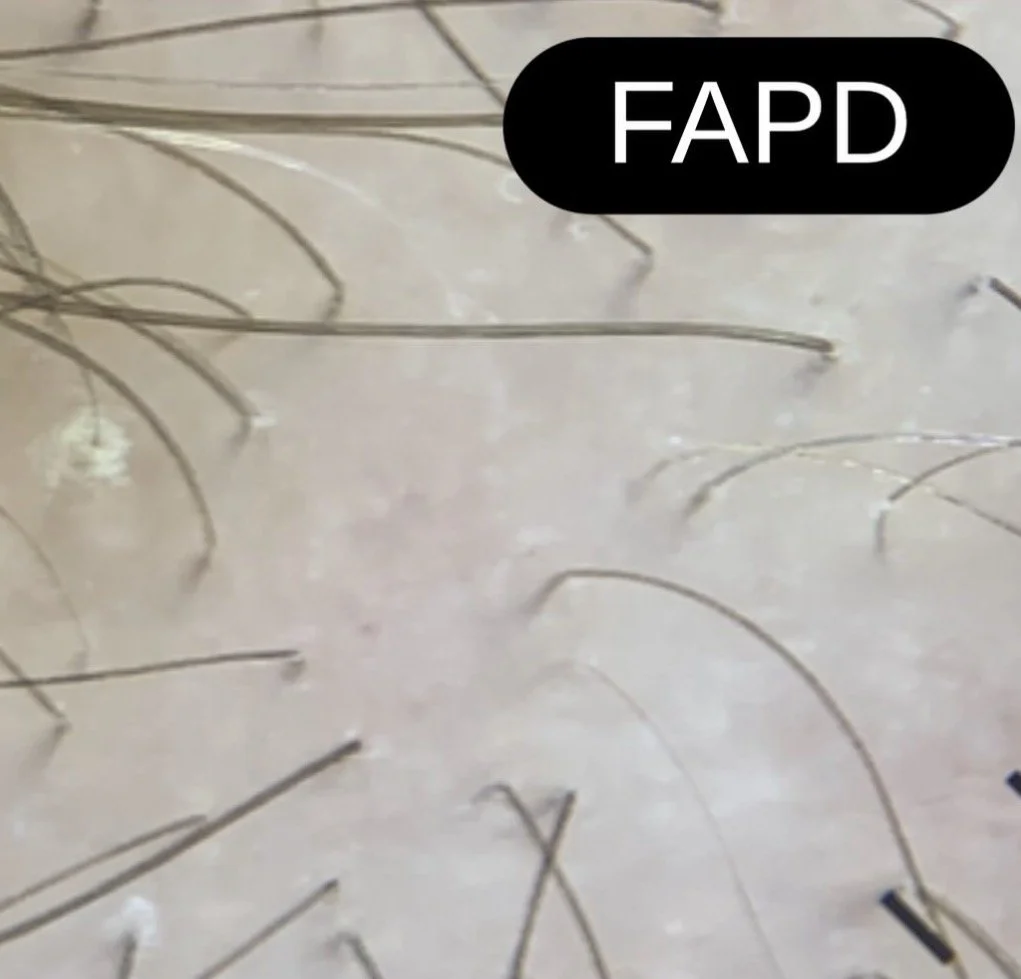
Not every man dressed in a red suit in the month December is Santa Claus. And not every patient with a dual diagnosis of lichen planopilaris (LPP) and androgenetic alopecia (AGA) has fibrosing alopecia in a pattern distribution (FAPD). Over the past few years, I’ve become increasingly concerned (to say it lightly) about a quiet shift in how FAPD is being diagnosed in the world. There is a growing tendency to label patients as having FAPD simply because they carry two diagnoses: lichen planopilaris (LPP) and androgenetic alopecia (AGA). But this is not what FAPD is. So this trend is wrong. FAPD is not merely the coexistence of LPP and AGA. It is a distinct clinicopathologic entity. Patients with FAPD typically show:1) A symmetrical, patterned distribution of hair loss (often central scalp)2)A presentation that mimics AGA—but behaves differently3) Loss of vellus hairs with relative preservation of many isolated terminal hairs4) Subtle but important signs of inflammation, including perifollicular scale or erythema In contrast, classic LPP more often produces patchy, irregular areas of scarring hair loss. The introduction of the concept of discordant anisotrichosis by Saber et al in 2026 has been an important step forward. In typical AGA, hair shaft variability follows a relatively uniform and predictable progression. In FAPD, however, the variability is less than what is expected for the amount of density reduction. This feature provides a practical clue that something more than AGA is occurring. FAPD is not common—and it should not become a default label of AGA+LPP. Cases of FAPD have skyrocketed- and many diagnoses are wrong. The image shown here highlights some key features of FAPD. There is discordant anisotrichosis. Many follicular units contain single terminal hairs. Vellus hairs are not seen. Subtle perifollicular inflammation and scale can also be appreciated. Source link

Top Gift Ideas For People With Migraine
This post may contain affiliate links. Migraine Strong, as an Amazon Affiliate, makes a small percentage from qualified sales made through affiliate links at no cost to you. With the holiday season quickly approaching, gift shopping is officially on the horizon. Finding the perfect present for someone you care about can feel overwhelming—especially when you’re not quite sure what they want or what might truly help. The good news? We’re here to make celebrating, supporting, and choosing a meaningful gift for someone living with migraine a whole lot easier. We’ve curated thoughtful ideas designed to bring a genuine smile to your loved one’s face. Many retailers are already kicking off their holiday deals, and whenever possible, we’ll also share special Migraine Strong discount codes to help stretch your budget a little further. Keep an eye out for savings as you explore the list! To take the stress out of holiday shopping, we’ve gathered a selection of gifts that are both practical and comforting—great for anyone navigating migraine disease (including yourself!). Our hope is that this collection of top picks helps simplify your search and makes your gift-giving feel effortless, meaningful, and successful. 1. Migraine care package options Migraine gift bundles are a heartfelt way to show compassion and genuine understanding for the people you care about. Because you can tailor these care packages to match someone’s specific symptoms and needs, they’re a meaningful way to say, “I see what you’re going through, and I want to help.” To make your gift-giving effortless, we’ve gathered some of the most helpful tools and comforts that many people with migraine rely on. These migraine-friendly picks include items that can ease triggers between attacks and offer soothing relief during an attack—thoughtful gifts anyone living with migraine would be grateful to receive. Ear Plugs Nausea and Pain Relief Saje Peppermint Halo This is perfect for rolling directly onto the scalp to help ease head pain—and it’s truly one of my favorites. I love applying it around my hairline for that cool, icy sensation that wraps around my whole head. It’s a great source of distraction and comfort while waiting for medication to kick in! Peppermint Essential Oil Roll On is great not only for nausea but to mask strong triggering scents. Be Kool soft gel sheets – Great for symptom relief. Soothing Sleep Bucky 40 Blinks No Pressure Eye Mask – This eye mask blocks out every bit of light, all without putting pressure on your eyelids. It also helps keep your eyes comfortably moisturized throughout the night, making it a great option for more restful sleep. Alaska Bear Sleep Mask – This eye mask ensures no pressure on the eyes. Science Based Supplements Travel Pill Organizer – My favorite travel organizer for my bag. I use the 8 compartments to keep my migraine meds and acute cocktails with me, organized and labeled! Personal pampering TheraGun Mini Plus Massage Gun by Therabody – Handheld massager designed for travel or home. Helps ease migraine neck and shoulder pain. Ice Face Roller Massager – De-puff eyes and reduce migraine pain and you can customize it to include anything soothing for you. Tangle Teezer Plant-Based Ultimate Detangler Brush – This Tangle Teezer hair brush has regular-flex teeth that gently detangle straight to curly strands and is great for migraine sensitive scalps. Therabody SmartGoggles Heated Eye Mask – This mask offers customized treatments to lower heart rate, relieve eye strain or tension, provide headache/migraine relief and stress relief. Very soothing! Naturium The Glow Getter Multi-Oil Hydrating Body Wash – This hydrating body wash transforms from a luscious oil to a gentle lather, cleansing without stripping the skin of essential moisture. I love that it is unscented!LISAPACK Metal Eye Cream Roller Wand – This metal eye-roller wand can massage the eye and face to relieve eye strain, reduce puffiness, dark circles, wrinkles, and tighten skin. It’s lovely and cool when applying eye cream. Love it!Supergoop! Unseen Sunscreen – SPF 40 – This sunscreen is a totally invisible, weightless, scentless formula that provides oil-free sunscreen protection for all skin types and tones. Everyone in my family uses this and loves the feel and protection it offers. Will not leave a cast on the skin!Aquaphor Repairing Hand Masks – Hydrating and conditioning hand treatment infused with a blend of avocado oil and shea butter, plus Aquaphor’s signature ingredients. Unscented as well!! I love using these in the winter when my hands get so dry. Migraine Strong Amazon Store Thoughtful Gifts That Costs No Money An offer to watch the kids, walk the dog, throw in a load of laundry etc. to allow your loved one to rest would be well received & appreciated! Prepare dinner and pop it into their freezer so they have easy access to a healthy meal when they’re feeling their worst. Weighted products Nodpod Weighted Sleep Mask – Nodpod’s strap-free design evenly spreads gentle, deep-touch pressure across key points on the face, helping to calm a busy mind, soothe head pain, and ease you into deeper, more restful sleep. Nodpod Weighted Pod For Your Bod – It’s like having all the calming benefits of a weighted blanket wrapped into a single, convenient pod. Nodpod BODY’s unique design offers a cooler, more contouring experience, giving you the soothing feel of a full-sized weighted blanket in a portable, machine-washable form. Hand-Knit Weighted Blanket for Adults,Chunky Knit Blanket – carefully balanced weight distribution, this blanket drapes naturally with 8–12 pounds of gentle pressure. The deep-touch stimulation helps promote relaxation, making it easier to drift into a deep, restorative sleep. Cozy Comforts Women’s Pajamas Long Sleeve Sleepwear – These cozy PJ’s are perfect for lounging! Women’s Fuzzy Socks – The moderate thickness of these socks is nice for wearing during sleep or lounging.Chunky Knit Throw – This throw is cozy and warm. It has replaced my heated throw for the fall season! Crafts and Hobbies Crafting and hobbies can be a powerful distraction from the pain and discomfort of migraine. We

Aging with Dignity and Finding New Purpose While Living with Chronic Pain
At the age of 54, I began a journey in life that I never imagined would be mine to take on. After years of living with unexplained pain, experiencing strange reactions to food or medications, and frequently finding myself getting hurt with simple movements, I was finally diagnosed with a condition I had been born with called Ehlers-Danlos syndrome. I was relieved when a doctor figured out what was wrong, but then, after going home and reading about this condition being progressive and incurable, I went from excitement that I would finally fix myself to wondering how I was supposed to endure this for the rest of my life. When any of us is faced with chronic pain, we have to find a way to first mourn our losses and then, in time, figure out how to pick up the pieces and try to move on. I thrive, as I am guessing you do, when I feel that I have purpose and meaning in life. I had loved what I felt was my purpose: Being a mother to four sons, in a happy marriage, working as a middle school teacher, living on a small family farm with many animals. I was a high school swim coach and master swimmer, a gardener, a lover of reading, taking trips to the ocean, walking on the beach—and so much more. But as my condition progressed, many of those joys began leaving my life. I had too many procedures and too much pain to continue to be able to be effective in the classroom. I had to learn to cope with being reactive to certain foods and medications, and facing surgery after surgery to try to correct the damage my defective collagen created. I had to adjust to four years living in a wheelchair. The tendency of my joints to sublux, or partially dislocate, and the pain in my neck made walking on the sand, reading a book, and even chewing painful. But I still had a life to live. And I had a decision to make: Do I wallow in all this and let Ehlers-Danlos define me, or do I find a way to regain a new purpose and meaning in my life? It is daily work to try to feel purpose when you are confronted with conditions that cause chronic pain. The disruptions in your life can be heartbreaking, but at some point, you have to accept that this is the new version of your life. What can you do to help you find fresh purpose and meaning in your life? I have replaced so much of what I found pleasure in doing with new adventures. I joined the U.S. Pain Foundation initially as an advocate, and eventually became co-director of Cannabis Advocacy along with my husband. I learned to use my voice in my state and even in Washington, D.C., to speak out about issues I have a passion for. I work alongside others in our community with an Ehlers-Danlos syndrome support group to help pass along information we have learned that might help others cope with this under-recognized condition. I have adjusted my swimming strokes and technique due to my fused neck and limited mobility in my arms, but I am still in the pool, feeling the joy of the water and exercise. I know my sons are watching how I am taking on these challenges. I want them to respect me and understand that no matter what comes of their lives, if we work hard enough, we can still find joy and happiness. Your plans may not be the same as they used to be, but it’s still worth it to make new ones. May you find the strength to live your life with dignity as you, too, age with your chronic pain. It’s not easy, but there are many out there rooting for you! May life be kind to you… —by Ellen Lenox Smith Source link

Facts About Eosinophilic Esophagitis (EoE)
Español May 22, 2026, is World Eosinophilic Esophagitis (EoE) Day. More than 470,000 people in the United States are living with eosinophilic esophagitis (EoE), a condition that was once considered rare but has gotten more and more common over the last two decades. Knowing what EoE is can help you figure out whether it may be affecting you. What is eosinophilic esophagitis (EoE)? EoE is a chronic (long-term) immune condition that affects the esophagus, the tube that connects your mouth to your stomach. EoE happens when a type of white blood cell called an eosinophil builds up in the lining of this tube. The buildup causes chronic inflammation (swelling) in the esophagus that can lead to symptoms of EoE. What causes EoE? When a person has EoE, their immune system floods the esophagus with white blood cells as a response to triggers such as certain food and environmental allergens, touching the lining of the esophagus. This abnormal response by the immune system is known as Type 2 inflammation. Allergens like pollen, mold, dust and animal hair can trigger EoE. But the main cause of EoE are immune reactions to food. Foods that can trigger EoE include: Dairy products Peanuts and tree nuts Wheat Seafood/shellfish Eggs Soy Note: Not everyone with EoE reacts to the same foods, and testing cannot reliably predict which foods are triggers. What are the symptoms of EoE? EoE looks different at different ages. Babies and young children may not want to eat and may spit up or vomit more frequently, have stomach pain, have disrupted sleep, and not grow properly. For older kids and adults, the main symptoms of EoE are: Trouble swallowing Food getting stuck in the throat after swallowing (impaction) Heartburn Chest pain Stomach pain Food coming back up after swallowing (regurgitation) These symptoms may come and go, flaring up only once in a while, or they may be constant. Even when you don’t have symptoms, you still have EoE because it is a lifelong, chronic condition. Read: When My Son Was Diagnosed With EoE, Our Family’s World Was Turned Upside Down >> Who is affected by EoE? EoE can affect anyone at any age, but certain risk factors may make a person more likely to have the disease. Your chances of having EoE are higher if you have: Food allergies Environmental allergies (pollen, dust, animal hair, etc.) Asthma Hay fever (allergic rhinitis) Eczema or other skin conditions that cause itchy, inflamed patches A family history of EoE or other allergic conditions How do you diagnose EoE? Because the symptoms of EoE are similar to those caused by other health problems that affect the esophagus, like gastroesophageal reflux disease (GERD) or a food allergy, it can be tricky to diagnose. If your healthcare provider (HCP) thinks you may have EoE, they will send you to a gastroenterologist (GI doctor), which is a doctor who diagnoses, treats and manages diseases of the digestive system. They will look at your symptoms and do some tests, which may include: Upper endoscopy and biopsy: A long, skinny tube (endoscope) with a light and camera are used to view the lining of your esophagus and take samples to view under a microscope. An endoscopy and biopsy are required for an EoE diagnosis. Blood tests: Blood work is done to check for allergens, higher than usual eosinophil counts or other signs of allergic reactions. Note that blood tests alone cannot reliably diagnose EoE or food triggers. Esophageal sponge: A tiny sponge attached to a string is used to sample tissue in your esophagus without doing an endoscopy. How do you treat EoE? While there is no cure for EoE and it is a lifelong, chronic disease, it can be treated. Gastroenterologists treat and manage EoE. Allergists may also be part of your care team. While they cannot diagnose or treat EoE itself, they can help manage conditions that co-exist with EoE, such as food allergies. The best treatment for you depends on your unique health situation. Some of the treatment options for EoE are: Diet changes like cutting out certain foods that could trigger EoE. Proton pump inhibitors (PPIs), which are medicines that lower the amount of acid your stomach makes. Steroids, which are medicines that help reduce inflammation. EoE is treated using liquid steroids that are swallowed so they come in direct contact with the lining of your esophagus to take down swelling. Biologics (monoclonal antibodies), a type of treatment that targets certain cells or proteins linked to inflammation, which reduces inflammation and improves swallowing. Esophageal dilation, a procedure that involves using an endoscopy to widen the esophagus to make swallowing easier, but does not treat the underlying inflammation. Dilation is usually used along with medications or dietary changes. Treatments may change over time as your response and/or lifestyle change, so you should re-evaluate your treatment options with your HCP frequently. Since symptoms alone cannot determine whether you’re responding to treatment, repeated endoscopies and biopsies will be needed to measure your response to treatment and disease activity or progression. Together, you and your HCP can come up with a plan to treat your EoE on an ongoing basis. Living your best life with EoE If you think you may be having EoE symptoms — particularly if you also have allergies, asthma or other conditions that may put you at risk — talk to your HCP. Catching EoE early helps prevent damage to your esophagus that can happen over time. And the sooner you get a diagnosis, the sooner you can start managing your EoE so you feel better. This educational resource was created with support from Regeneron, Sanofi and Takeda. From Your Site Articles Related Articles Around the Web Source link

Allegra & Pepcid for Anxiety—Doctors Explain TikTok Trend
If you purchase an independently reviewed product or service through a link on our website, SheKnows may receive an affiliate commission. Scroll through TikTok right now, and you’ll find women claiming that an unlikely over-the-counter combo—Pepcid AC and Allegra—has dramatically improved everything from PMDD symptoms to anxiety and depression. In videos racking up hundreds of thousands of views, users say the pairing helps take “the edge off,” quiet intrusive thoughts, reduce irritability, or ease the emotional volatility that can come with hormonal shifts and perimenopause. The trend is taking off in part because it taps into something very real: many women struggling with PMS, PMDD, anxiety, and hormonal mood changes feel underserved by the healthcare system and are desperate for relief. Premenstrual dysphoric disorder (PMDD), a severe form of PMS that can cause debilitating emotional symptoms, affects an estimated 3 to 8 percent of women of reproductive age, though experts believe it’s significantly underdiagnosed. Many women spend years being told their symptoms are “just stress,” regular PMS, or generalized anxiety before finally getting answers. Related story A New Old Navy x Disney Americana Collection Has Arrived & It’s Filled With Cute Matching Family Moments for Summer Pepcid AC Maximum Strength Heartburn Relief Tablets Allegra Adult 24-Hour Allergy Relief Tablets At the same time, women are nearly twice as likely as men to be diagnosed with depression, with recent CDC data finding depression prevalence rates of 16% in women compared to 10.1% in men. And hormonal fluctuations—from the menstrual cycle to postpartum changes to perimenopause—can play a major role in mood symptoms for many patients. So it’s perhaps not surprising that a TikTok trend promising relief from anxiety, mood swings, rage, or emotional overwhelm would quickly gain traction online. But can an allergy medication and an acid reducer actually help with mental health symptoms? According to experts, the answer is nuanced. “There’s an interesting theory behind this trend, but no real proof it works for mood,” says Pallavi Khanna, MD, an OB/GYN who works in Regional One Health’s Menopause Care Clinic in Memphis, Tennessee. The theory centers around histamine, the same chemical involved in allergic reactions. Estrogen can stimulate immune cells called mast cells, which release histamine throughout the body. Histamine doesn’t just cause sneezing, itching, or hives—it also acts as a neurotransmitter in the brain and may influence anxiety, inflammation, sleep, and stress responses. “So, if you block histamine on two fronts — Allegra blocks one type of receptor (H1), Pepcid blocks another (H2) — the thinking is that you might quiet the whole system down,” explains Dr. Khanna. Still, she cautions against confusing a plausible biological theory with proven treatment. “As I tell my patients, ‘biologically plausible’ is not the same as ‘actually works.’” What Pepcid AC and Allegra Actually Do As mentioned, Pepcid AC contains famotidine, an H2 blocker originally designed to reduce stomach acid production. Allegra, meanwhile, is an H1 antihistamine used to treat allergy symptoms like sneezing and itching. Together, some TikTok users believe the medications can “calm” the body’s histamine response and, in turn, improve mood symptoms tied to hormonal fluctuations. “Famotidine is a histamine-2 (H2) blocker that was designed to block acid production in the stomach,” says Karyn Eilber, MD, member of the plusOne Wellness Collective. “Other organs have H2 receptors, including the uterus and the brain, so Pepcid may help anxiety and menstrual cramps.” She adds that while the brain also contains H1 receptors, Allegra itself likely has less impact on anxiety because it doesn’t significantly cross the blood-brain barrier. “Fexofenadine is a larger molecule that is too big to cross the blood brain barrier (enter the brain) so it likely doesn’t have any effect on anxiety; however, smooth muscle like that found in the uterus also has H1 receptors so Allegra may help uterine cramps too.” Dr. Khanna agrees that histamine may play some role in the physical symptoms associated with hormonal shifts, especially in perimenopause, when fluctuating estrogen levels can intensify everything from bloating to sleep issues to skin reactions. But she says histamine likely isn’t the primary driver behind PMDD’s emotional symptoms. “When it comes to PMS and PMDD specifically, histamine isn’t the main character,” she says. “The leading explanation is that some women’s brains are unusually sensitive to a metabolite of progesterone called allopregnanolone.” She also notes that serotonin pathways are heavily involved, which is why SSRIs remain one of the most effective evidence-based treatments for PMDD. Unlike generalized depression, PMDD symptoms are cyclical and tied specifically to hormonal changes during the luteal phase of the menstrual cycle, which is why treatments often look different than standard anxiety or depression care. Why Some Women Say the Combo Helps Even without formal clinical studies, many TikTok users insist the medications are helping them feel calmer, less reactive, or more emotionally stable. According to experts, there are several possible explanations—and not all of them are necessarily “just placebo.” For one, improving physical symptoms can have a real downstream effect on mental health. PMS and perimenopause can cause bloating, GI issues, reflux, headaches, breast tenderness, flushing, poor sleep, and inflammation-like symptoms that make people feel physically miserable. Reducing those symptoms can indirectly help the nervous system feel calmer too. “When your body stops feeling inflamed, your nervous system calms down,” explains Dr. Khanna. Dr. Eilber echoes that idea, saying, “An indirect way that these medications can improve anxiety and emotional symptoms is that if you physically feel better then everything, including anxiety, is better.” There’s also the possibility that some women experiencing relief could have underlying mast cell activation issues, a condition involving overactive immune cells that can worsen with hormonal fluctuations. Dr. Khanna says she sees this more often than people realize in her perimenopause clinic. “Some women have mast cells that overreact, and estrogen makes those cells more reactive,” she says. “So as estrogen swings around the cycle or chaotically through perimenopause, they get flushing, hives, GI symptoms, weird sensitivities, and yes, anxiety that tracks [with] their hormones.” And then
Neutrophil-to-lymphocyte ratios (NLR) and Platelet-to-lymphocyte ratios (PLR) in Alopecia Areata — Donovan Hair Clinic
Every patient with hair loss needs blood tests. Surprisingly, some blood tests reveal more information than you might imagine! For example- a complete blood count (CBC) provides counts of red cells, white cells, and platelets and we can tell if a patient has various issues – like anemia. But there are some interesting information that might also be hidden in test results. Let’s talk about inflammatory indices such as the neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR). Higher values generally reflect a shift toward systemic inflammation. The exact cutoffs and significance is still being studied by researchers but NLR ratios above 3 seems to be concerning and PLR ratios that rise for a given patient over time may also be concerning (although exact cutoff values are less clear) In alopecia areata (AA), several case-control and cross-sectional studies report higher NLR and PLR in patients vs controls. More interestingly, some studies show stepwise increases with disease burden—patients with extensive disease (e.g., higher SALT scores, alopecia totalis/universalis) tend to have higher NLR and PLR than those with patchy AA. A few reports also link higher baseline NLR with longer disease duration and greater activity (e.g., positive hair-pull test), suggesting these ratios may reflect ongoing immune activation. There are also early signals on prognosis and treatment response. Small cohorts have found that lower baseline NLR may be associated with better response to therapies (including corticosteroids and JAK inhibitors), whereas persistently elevated NLR & PLR can track with refractory disease. However, these findings are inconsistent across studies and often lose significance after adjusting for confounders. Importantly, evidence comes almost entirely from small, observational studies with variable cutoffs and methods. There are no validated thresholds and no randomized trials confirming clinical utility. For now, NLR and PLR are best viewed as adjunctive, research-level markers—useful for understanding systemic inflammation in AA, but not reliable standalone tools for diagnosing, staging, or guiding treatment decisions. Source link

Training for a half marathon was not straightforward, just like my journey with migraine.
My first migraine attack happened when I was 14 years old and in school. My hand and mouth became numb, I had an intense headache, and I didn’t know what was happening. Nowadays, I can go up to six months of not having a migraine attack and then have a period of having migraine symptoms daily. My symptoms begin with blurry vision, it’s as if glass has shattered and I can’t read things. When this happens, I take painkillers early to manage my symptoms, but I still experience aura. I’m lucky in that if I catch it early enough, I can treat my symptoms with basic painkillers. Sometimes, my migraine attacks can come on suddenly, for example, when I’m looking after my kids. When this happens, I need to take time out and sit in a dark room. When this occurs, I’ve had to stay in bed for the rest of the day and not interact with anyone. Source link