
by Dr Elissa Dabaghi (Frontline Gastroenterology Global Taskforce 2025-6) Colorectal cancer remains one of the most prevalent causes of cancer-related deaths in the United States, where geographic location can significantly affect whether appropriate colorectal cancer care is available. Individuals living in low socioeconomic status areas have about a 37% higher risk of colorectal cancer and a 24% higher risk of cancer-related death than those living in higher socioeconomic status areas. Given the rapid integration of artificial intelligence into medicine, we must assess its potential impact on health equity. As the use of artificial intelligence (AI) in medicine grows, will this technology bridge or deepen existing socioeconomic disparities in access to colorectal care? Rural healthcare demonstrates the critical need to bridge the gap in healthcare disparities. The number of practicing general surgeons in rural communities has declined rapidly. Meanwhile, specialists, including colorectal surgeons, predominantly reside in urban communities. The general surgeon workforce in rural areas is projected to drop significantly in the next decade, while the workforce in urban and metropolitan communities is projected to almost double. Furthermore, there are substantial geographic barriers for patients living in rural areas. Some statistics show that 1 in 5 Americans residing in rural areas live more than 60 miles from a medical oncologist. These trends directly threaten colorectal cancer screening and treatment, as general surgeons perform over 50% of screening colonoscopies in these rural areas. With the growing use of technology and the implementation of AI, many wonder whether AI can help bridge this gap in healthcare, particularly in colorectal care, with regard to screening for colorectal cancer and potentially surgical planning. New systems, such as GI Genius, can identify colonic polyps that can be easily missed by the human eye. Certain studies have shown that this technology can decrease the adenoma miss rate from 32.4% to 15.5% when AI is utilized, with improvement seemingly most apparent in non-expert endoscopists. This is critical for reducing colorectal cancer risk over 5 years and can have a significant impact on rural healthcare, which already has limited access to specifically expert endoscopists. These AI systems could therefore help to both train less-experienced endoscopists to achieve higher adenoma detection rates and, beyond that may serve as expert-level support during these screenings going forward. However, it is important to mention that even with the implementation of AI-assisted polyp detection during colonoscopy, endoscopists remain essential to ensuring these systems are utilized effectively and appropriately. Endoscopists must understand the limitations of AI, and avoid overreliance, but rather utilize this technology as an adjunct to clinical judgement and shared decision-making, as highlighted by Frontline Gastroenterology’s review (1). Another potential utility of AI and machine learning algorithms in rural or resource-strapped settings is to triage patients who require urgent referral to specialist centers. Some AI-based prediction models have succeeded in stratifying colorectal cancer patients by one-year mortality risk, allowing the streamlining of care for more urgent cases as well as the tailoring of appropriate perioperative care to each patient. Additionally, although patients in rural areas often already use telemedicine for remote consultations and office visits, it could be interesting to pair AI with diagnostics in this setting. Patients in these rural areas who require endoscopic screening could choose to undergo a capsule endoscopy that integrates AI and machine-based polyp detection at their local center. This would ultimately facilitate more convenient (and likely, by extension, timely) colorectal cancer screening for patients that may not have access to specialist centers. Despite its promise, it is important to acknowledge the potential of AI to widen gaps in US healthcare, either through financial barriers or by creating additional limitations on access to resources. Additionally, implementing the use of AI in a rural healthcare system could be challenging due to the substantial investments and costs required to roll and maintain such systems (at all levels of care). Not only are these communities already financially stretched, but they may also lack the essential resources required to operate this technology (such as platform upgrades and even high-speed internet). Furthermore, many diagnostic AI systems are trained on data from large urban populations, which could lead to higher rates of incorrect diagnostic readings for rural populations with different demographics. As discussed in an article by Frontline Gastroenterology, the reliability of AI-driven predictions is dependent on high-quality data input (2). This article emphasizes that reducing irrelevant data input and systemic bias through precise and rigorous data selection to properly train the algorithm is essential to developing predictive tools that genuinely benefit patients of all demographics. Finally, given the relative ease of implementing these AI systems in large, urban healthcare facilities, as opposed to rural settings, there is a potential for this technology to drive patients away from local already struggling rural hospitals to these centers. This can place further strain on the finances of these institutions, and ultimately potentially worsen healthcare accessibility through their closure. Finally, as things currently stand, healthcare insurance systems and Medicare do not offer differential reimbursement rates for the use of AI-assisted technology, which could represent a challenge for rural hospitals in generating the initial financial outlay required to deploy this technology. In conclusion, we must ensure that AI reduces and prevents the worsening of disparities in colorectal care, and healthcare in the US as a whole. This includes strengthening and training these algorithms on rural populations to prevent inequities in underserved areas, as well as ensuring adequate funding for AI-assisted care to be implemented in these rural hospitals, which already have limited resources. Overall, however, there is great potential for AI to augment, not replace, rural providers and enhance triaging patients, risk stratification, and access to expert and specialized support. References Olabintan O, Fearnley L, Iniesta R, et al. Artificial intelligence in endoscopy: navigating risk, responsibility and ethical challenges. Frontline Gastroenterology Published Online First: 17 November 2025. doi: 10.1136/flgastro-2025-103107 https://fg.bmj.com/content/early/2025/11/17/flgastro-2025-103107 Ashton JJ, Brooks-Warburton J, Allen PB On behalf of the British Society of Gastroenterology artificial intelligence in IBD special interest group, et al. The importance of

You are Not Your Pain: A Teen’s Perspective on Living With Chronic Illness
By Nayeli R. Hevezi Chronic pain will always be frustrating and exhausting. However, the pain shouldn’t make us lose sight of the beauty around us. With the current state of the world, it’s hard to look for the little things that make what’s going on less scary, especially when you have chronic pain. A flare-up plus global warming? No, thank you! Teenagers with chronic pain tend to have our lives planned around our pain. We constantly have to make sure that we are feeling strong enough or well enough to partake in activities and participate in normal teenage things. But recently, I have found that my pain doesn’t define me. You’re allowed to have fun and live your life with joy and happiness. You shouldn’t have to sacrifice your own happiness and enjoyment for your pain. For example, I recently finished writing my debut novel, Annotation, which revolves around two teenagers, one of whom has chronic pain. The book is a rom-com but also ties in what it’s like to be a teenager with chronic pain. It shows how even with the pain we experience, it doesn’t mean we have to stop looking for the light in the world. I wrote this book as a way to cope with my own pain and feelings regarding being a teenager and dealing with chronic pain, and it is my hope that my book can reach other teenagers who can relate and find a safe escape within my book. In addition to my book, in autumn of 2024 I created a book account on Instagram. I created it after seeing many teenagers post about books and shared interests. I decided to join the book community on Instagram as a way to post about my own interests and to meet other like-minded individuals. And much to my delight, I have met hundreds of people because of my book account. I have found real friends who support me and never fail to make me laugh. Along with those friends, I have also found friends who have chronic illnesses and experience similar chronic pain to me. We are able to connect on so many levels, which makes our friendship feel deeper and more meaningful. I have found that even just talking to them for a few minutes can turn a bad day into a good one. Having friends who are able to empathize with what we experience is always a heartwarming feeling. Research regarding chronic pain is nowhere close to where it needs to be. As teenagers who are already dealing with enough stress in our lives, having that extra pain completely wears us out, so having one or two good friends who are able to be there for you when you’re in pain is amazing! Our pain does not need to overshadow the sweetness in our lives. Finding hobbies that distract you or allow you to cope with your pain may end up turning into a passion of yours, and hopefully you can allow some whimsy into your life. —by Nayeli R. Hevezi Source link

Información comprobada de la esofagitis eosinofílica (EEo)
English El 22 de mayo de 2026 es el Día Mundial de la Esofagitis Eosinofílica (EEo). Más de 470,000 personas en Estados Unidos viven con esofagitis eosinofílica (EEo), un trastorno que alguna vez se consideraba infrecuente pero que se ha vuelto cada vez más común en las últimas dos décadas. Saber lo que es la EEo puede ser útil para determinar si te está afectando. ¿Qué es la esofagitis eosinofílica (EEo)? La EEo es un trastorno inmunitario crónico (a largo plazo) que afecta el esófago, es decir, el conducto que conecta tu boca con tu estómago. La EEo ocurre cuando un tipo de glóbulo blanco denominado eosinófilos se acumula en la mucosa de este conducto. Esta acumulación causa inflamación (hinchazón) crónica en el esófago que puede causar los síntomas de la EEo. ¿Cuál es la causa de la EEo? Si una persona tiene EEo, su sistema inmunitario inunda el esófago con glóbulos blancos como una reacción a desencadenantes tales como ciertos alimentos y alérgenos ambientales que tocan la mucosa del esófago. Esta reacción anormal del sistema inmunitario se conoce como inflamación tipo 2. Alérgenos tales como polen, moho, polvo y pelos de animales pueden desencadenar la EEo. Pero reacciones inmunitarias a alimentos son la causa principal de la EEo. Los alimentos que pueden desencadenar la EEo incluyen: Productos lácteos Manies y frutos secos Trigo Pescados y mariscos Huevos Soya Nota: No todas las personas que tienen EEo tienen reacciones a los mismos alimentos y las pruebas no pueden predecir en una forma confiable qué alimentos la desencadenan. ¿Cuáles son los síntomas de la EEo? La EEo es diferente a edades distintas. Los bebés y los niños pequeños podrían no querer comer y podrían escupir o vomitar más frecuentemente, tener dolor de estómago, tener alteraciones de sueño y no desarrollarse apropiadamente. Para niños más grandes y adultos, los síntomas principales de la EEo son: Dificultad para tragar Alimentos que se atoran en la garganta después de tragarlos (impactación) Acidez Dolor de pecho Dolor estomacal Alimentos que suben después de tragarlos (regurgitación) Estos síntomas podrían ser intermitentes, aparecer cada cierto tiempo o ser constantes. Incluso si no tienes síntomas, podrías tener EEo porque es un trastorno crónico y de por vida. Lee: Cuando le diagnosticaron EEo a mi hijo, el mundo de nuestra familia se puso de cabeza >> ¿A quién le afecta la EEo? La EEo puede afectar a personas de cualquier edad, pero ciertos factores de riesgo podrían hacer que una persona sea más propensa a tener ese trastorno. Tus probabilidades de tener EEo son mayores si tienes: Alergias alimentarias Alergias ambientales (polen, polvo, pelos de animales, etcétera) Asma Rinoconjuntivitis (rinitis alérgica estacional) Eccema u otros trastornos cutáneos que causan manchas con picazón e inflamación Antecedentes familiares de EEo u otros trastornos alérgicos ¿Cómo se diagnostica la EEo? Puesto que los síntomas de la EEo son similares a los de otros problemas médicos que afectan el esófago, tales como enfermedad por reflujo gastroesofágico (ERGE) o alergias alimentarias, puede ser difícil diagnosticarla. Si tu proveedor de atención médica (HCP, por sus siglas en inglés) piensa que podrías tener EEo, te referirá a un gastroenterólogo (doctor GI), que es un doctor que diagnostica, trata y controla trastornos del sistema digestivo. Evaluará tus síntomas y hará algunas pruebas, las cuales podrían incluir: Endoscopía superior y biopsia: Una sonda larga y delgada (endoscopio) con una luz y una cámara se usan para visualizar la mucosa de tu esófago y tomar muestras para verlas bajo un microscopio. Se requiere una endoscopía y una biopsia para el diagnóstico de EEo. Análisis de sangre: Se realizan pruebas de sangre para detectar alérgenos, cantidades anormalmente altas de eosinófilos y otras señales de reacciones alérgicas. Toma en cuenta que análisis de sangre en forma individual no pueden diagnosticar con certeza la EEo o identificar desencadenantes alimentarios. Esponja esofágica: Se usa una esponja pequeña adherida a un hilo para tomar muestras en tu esófago sin realizar una endoscopía. ¿Cómo se trata la EEo? Si bien la EEo es un trastorno crónico de por vida que no tiene cura, puede tratarse. Gastroenterólogos tratan y controlan la EEo. Alergólogos también podrían ser parte de tu equipo médico. Si bien no pueden diagnosticar ni tratar la EEo en sí, pueden ayudar a controlar trastornos que coexisten con la EEo, tales como alergias alimentarias. El mejor tratamiento para ti depende de tu situación médica específica. Algunas opciones terapéuticas para la EEo son: Cambios dietéticos tales como reducir el consumo de ciertos alimentos que podrían desencadenar la EEo. Inhibidores de la bomba de protones (IBP), los cuales son medicamentos que reducen el monto de ácido que tu estómago genera. Corticoides, los cuales son medicamentos que son útiles para reducir la inflamación. La EEo se trata usando corticoides líquidos que se tragan para que entren en contacto directo con la mucosa de tu esófago para reducir la inflamación. Biofármacos (anticuerpos monoclonales), un tipo de tratamiento que se dirige específicamente a ciertas células o proteínas relacionadas con la inflamación, reduciéndola y haciendo que tragar sea más fácil. Dilatación esofágica, un procedimiento en el cual se usa un endoscopio para ensanchar el esófago para hacer que tragar sea más fácil, pero que no trata la inflamación subyacente. La dilatación normalmente se usa con medicamentos o cambios de dieta. Los tratamientos podrían cambiar con el tiempo a medida que tu reacción o estilo de vida cambie, por lo que deberías reevaluar tus opciones terapéuticas con tu proveedor de atención médica frecuentemente. Puesto que no se puede determinar si el tratamiento está funcionando en función exclusiva de los síntomas, se necesitarán endoscopías y biopsias en forma repetitiva para evaluar el tratamiento y la actividad o progreso de este trastorno. Tú y tu proveedor de atención médica, juntos, podrán determinar un plan para tratar tu EEo en forma continua. Disfrutar tu vida al máximo con EEo Si piensas que podrías tener síntomas de EEo, particularmente si también tienes alergias, asma u otros trastornos que incrementan tu riesgo, habla con tu

Important Announcement: Josie Roberts, CNM, Relocating
Farewell and Best Wishes for Our Midwife, Josie Roberts, CNM It is with both excitement and sadness that we share that our beloved midwife, Josie Roberts, CNM, will be relocating to the Pacific Northwest this September to follow her family’s dreams. Over the years, she has cherished walking alongside our patients through pregnancies, celebrating births, and catching up on life’s milestones. Her words capture it best: “Your strength and endurance are awe inspiring!” While she will be deeply missed, rest assured your care at Adriatica Women’s Health will continue without interruption. Our midwife team, or any Adriatica Women’s Health provider of your choice, will be happy to continue caring for you. If you wish to transfer your care outside our practice, you may request a medical records release form at www.adriaticawomenshealth.com or through our office. For any questions, please contact us at 972-542-8884. From all of us at Adriatica, we thank her for her years of dedication and wish her and her family the very best in this exciting new chapter. Click here to read Josie’s letter to her patients. Source link
Stopping JAK Inhibitors in Pregnancy — Donovan Hair Clinic
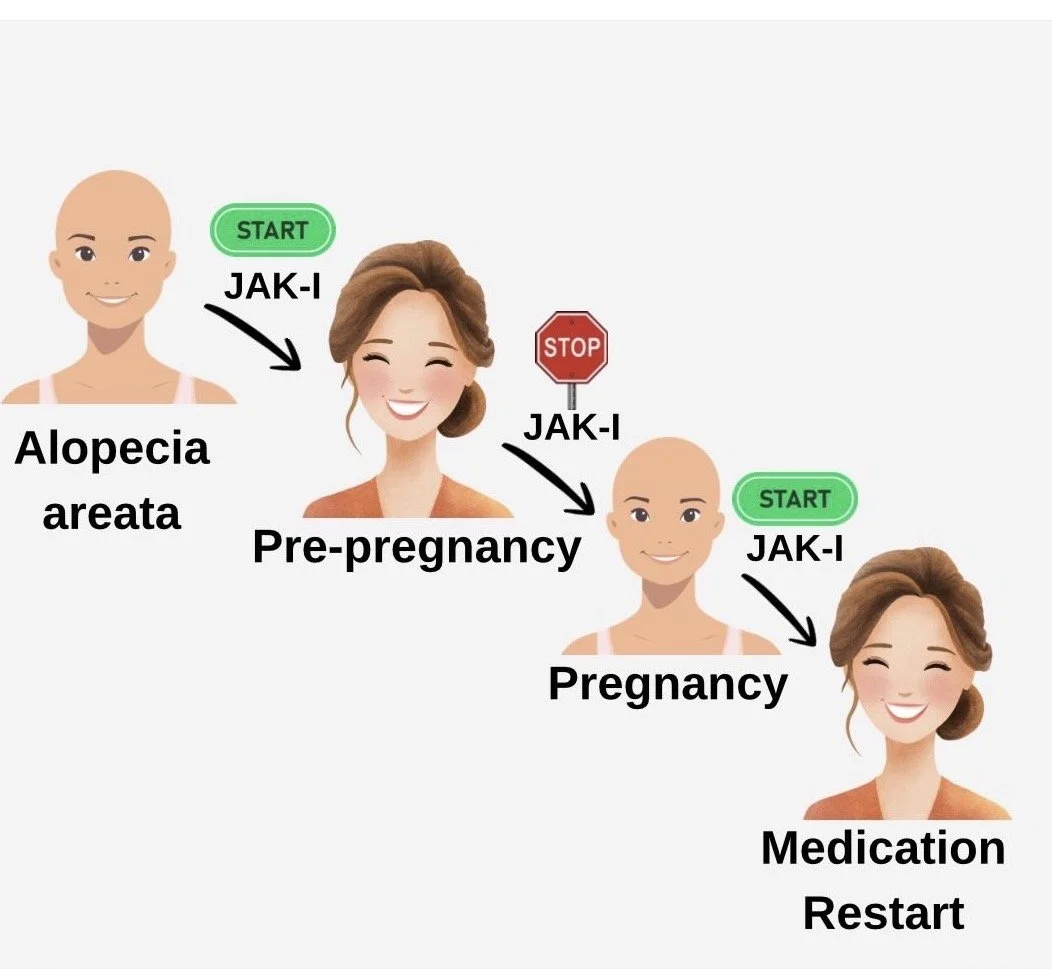
Janus kinase inhibitors (JAK inhibitors) are medications that can help some patients with severe alopecia areata (AA) regrow hair. But because safety in pregnancy isn’t fully known, current recommendations are for all women stop treatment when trying to conceive. Unfortunately, this usually leads to hair loss. A nicely conducted new study set out to describe what happens to scalp hair when women stop JAK inhibitors for pregnancy — and what happens after restarting them postpartum. Researchers followed 9 women with severe AA through 14 pregnancies. All stopped oral JAK inhibitors before or early in pregnancy. RESULTS Every woman experienced significant hair loss after stopping treatment. However, once JAK inhibitors were restarted — usually within 4 months after delivery — patients regrew their hair, often back to or better than before. CONCLUSIONS This study is great news for the many women with alopecia areata who want to become pregnant but are terrified to stop their JAK inhibitor. Women with AA who must stop JAK inhibitors during pregnancy should be counseled that hair shedding is highly likely. The encouraging news is that restarting treatment after delivery (and after breastfeeding is done) led to meaningful regrowth in all cases. This study highlights the emotional burden these women face and the need for clearer pregnancy-related treatment guidelines in AA. REFERENCE Ogbutor C et al. Int J Womens Dermatol. 2025;11:e218 Source link

From research lab to medicine cabinet: how new migraine treatments are discovered
The first widely used migraine-specific treatments, the triptans, were introduced in the early 1990s. These drugs marked a turning point towards more targeted management of migraine. However, a substantial proportion (around one third) of individuals do not respond adequately to current treatments. Many drugs primarily target head pain, despite non-pain symptoms like fatigue, light sensitivity and nausea often being just as debilitating. As a result, researchers continue to search for new drug targets. But how does a new migraine treatment turn from an idea into something prescribed in a clinic? This blog will give you some insights into what happens ‘behind the scenes’ of drug discovery. Where do new ideas come from? New treatment ideas begin with discovery science. As research improves what we know about what’s happening in the brain during a migraine attack, scientists identify biological processes that could be targeted with drugs. For example, Calcitonin Gene-Related Peptide (CGRP) was discovered to play a key role in migraine pain-signalling as its levels were shown to increase in people during attacks. This initial insight led to the development of therapies to block its effects, with some drugs now available. But not all scientific discoveries lead to the development of new drugs. Sometimes researchers can repurpose existing treatments, like botox, instead. In other cases, observing the strengths and weaknesses of existing drugs, helps researchers design safer or more effective options. New treatments rarely emerge in isolation but instead build on decades of accumulated research and clinical observations. From the research lab: Once an idea is generated, the earliest stage of drug development happens in laboratories. Scientists will first test compounds in preclinical models, like cells, animals or computer simulations, to look for signs that one of these compounds might improve migraine-related biology. You can think of drug discovery as testing many different keys in a complex lock (which may itself not yet be understood). If a particular compound is successful at improving migraine-related biology, it becomes a potential new medicine, known as a ‘drug candidate’. However, scientists may need to test thousands of compounds before finding one promising drug candidate, making this a challenging and time-consuming process. These initial investigations done in preclinical models allow researchers to begin to assess both how effective a drug candidate is at modifying migraine-related biology and whether it appears safe enough to progress further. To the medicine cabinet: If a medication shows promise in preclinical testing, it will move on to clinical trials. Clinical trials are divided into four phases to ensure safety of participants and effectiveness of a drug. Each phase has its own specific purposes and builds upon the preceding phase. The key questions answered and goals of each phase of a clinical trial are as follows: Phase 1: Is it safe? What dose should be used? Small groups of healthy participants are studied to determine the safety of the drug candidate. Phase 2: Does it show signs of working? Is it effective in improving migraine biology in people with migraine? Larger groups of volunteers, including people with migraine, allow researchers to test the effectiveness of the drug at improving migraine-related biology. Phase 3: Does it work well and safely compared to existing treatments? Does it provide additional benefits to existing drugs that are already on the market? Large populations are studied to assess if there are improved benefits to most people with migraine. Approval by regulatory bodies: Can this drug be put on the market? If there is evidence that a drug candidate meets these criteria in a significant proportion of participants, the medication will be considered for market approval. In the United Kingdom, regulatory bodies like the Medicines and Healthcare products Regulatory Agency (MHRA) oversee the approval of new medications. These regulatory bodies are critical in ensuring treatments are safe and effective for public use. In England and Wales, approval by regulatory bodies is not the final stage. New drugs also need to be assessed and approved by the National Institute for Health and Care Excellence (NICE) to make them available to people being treated by the NHS, often with specific rules. Phase 4: What happens after approval in real-world use? Even after approval, drugs continue to be monitored. This is done to look out for rare side effects that may not have been spotted during clinical trials. It also allows real-world data to be collected to refine how medications are used. For example, drugs could be repurposed or better dosing strategies can be discovered to improve their use in migraine management. Why does this process take so long? It can take years (and hundreds of millions of pounds) to develop an idea for a new migraine medication into a fully-fledged drug that is prescribed in the clinic. Circling back to the development of the triptans, although they were discovered in the late 1970s, they were only made available to the public in the 1990s. Similarly, CGRP was initially discovered in the early 1980s and convincingly linked to migraine biology in 1990, but the first CGRP-targeting drug (a CGRP monoclonal antibody called erenumab) was only approved for use in 2018. Testing these medications for safety and effectiveness took around 20 to 30 years, highlighting that the process from drug discovery to development can be slow. Many potential drugs fail along the way either in their ability to work well in improving symptoms of a migraine attack, in their safety or in providing more benefits than existing medications. Therefore, time is needed to ensure that beneficial medications are being developed. What is currently in the discovery pipeline? There are currently exciting prospects in the migraine treatment pipeline. While much progress has been driven by targeting CGRP, researchers are now exploring new approaches that go beyond pain. Recent clinical trial data showed the potential for early intervention in migraine care, whereby blocking CGRP signalling during the earliest phase of an attack, prior to the onset of pain demonstrated beneficial effects. Data from the study suggests that the early use of a
Changing course: Recognize signals, understand science
Column Orthopedics Today Commentary Add topic to email alerts Receive an email when new articles are posted on Please provide your email address to receive an email when new articles are posted on . “ data-action=”subscribe”> Subscribe We were unable to process your request. Please try again later. If you continue to have this issue please contact customerservice@slackinc.com. Back to Healio More from Column Orthopedics Today Commentary View all The challenges of health care have led many physicians to consider changing their professional environment. The first impulse is to modify the current situation, but systemic and institutional inertia may prevent any meaningful change. Questions arise and these concerns may be briefly silenced by strong clinical outcomes, patient gratitude or the rewards of mentoring fellows and residents who value your guidance. However, for an increasing number of physicians at every stage of a career, the introspective voices may be growing louder, leading one to question if status quo is still acceptable or if it is time to change course. These questions are not signs of weakness, loss of resilience or ingratitude. They reflect professional clarity and alignment with priorities and, increasingly, survival. Burnout rates among physicians have risen sharply during the past decade. The corporatization of medicine, loss of clinical autonomy, escalating administrative burdens and a sustained erosion of the patient-physician relationship have contributed. For younger physicians, disillusionment can arrive before a strong foundation is established. For mid-career physicians, recognizing that a current environment cannot fulfill their long-term vision can feel paralyzing. For senior physicians, early retirement becomes an increasingly appealing alternative. Not a failure Changing course is not failure. When approached with clarity, evidence and intention, it is often the most courageous and consequential professional decision a physician can make. The most effective way to consider a career change begins long before a moment of crisis. Every physician should develop a personal vision and mission statement that integrates professional and family priorities. This can be a dynamic document that articulates your professional vision, how you want to prioritize your time, and what matters most to your family. Ideally grounded in enduring principles, it can be refined as life stages, relationships and family circumstances change. When this foundation exists, decisions become measurable. You can honestly ask if your current environment is moving you toward or away from stated values. When the answer is consistently away, the stages of change have already begun whether recognized or not. Stages of change The Transtheoretical Model of behavior change provides a validated framework for understanding how physicians navigate professional transitions. It identifies six stages: precontemplation, contemplation, preparation, action, maintenance and termination. Every major career pivot aligns with this model. In the precontemplation stage, a physician has not yet recognized a problem. Performance remains high, external recognition is strong and dissatisfaction is rationalized as temporary. Sentinel events that move a physician into contemplation include leadership transitions, gradual erosion of input in institutional decisions, diminished autonomy and a growing dissonance between personal values and organizational expectations. Moral distress deserves particular attention. It is not frustration or a lack of resilience. It is a documented psychological red flag arising from a persistent mismatch between a physician’s clinical values and system demands. If unaddressed, it predicts emotional exhaustion, depersonalization and departure from the organization on the organization’s terms rather than the physician’s own terms. In contemplation, the physician gathers information, strengthens networks and relationships, and consults legal and financial experts. If change is pursued, then action leads to the transition, followed by maintenance, the critical post-transition stabilization period, and finally termination, which marks full integration into a new environment. The central lesson is not to wait for a crisis. When multiple red flags converge, preparation should begin on the physician’s terms. Structured introspection is the most powerful instrument in any career decision. The strongest predictor of a successful transition is clarity about one’s vision. Ask whether you are building the skills, relationships and reputation that reflect who you want to be in a decade. Without a vision, decisions default to reactivity. Equally important is a structured evaluation of the trade-offs of staying vs. changing. Life stage Career mobility is profoundly shaped by life stages. In the early years, mobility is the highest and the cost of redirecting is lowest. A physician who discovers that a clinical environment does not align with their vision should act early and decisively, before a mature practice and referral base are established and contractual obligations mount. Clarity about what you do not want is as valuable as clarity about what you do. In mid-career, mobility carries real cost. A mature referral network, established relationships with hospitals and ASCs, and ties to your community and school-aged children are powerful anchors. Transitions must be carefully planned, as referral bases are rarely transplanted and financial costs are measurable. However, cost does not mean wrong. In late career, the risk calculus shifts. Children are leaving home, financial security is more established and one’s professional reputation has matured. However, it is important to recognize that relocating to a different region offers limited portability of a mature referral network. Among professional peers, reputation is more transferable, and leadership roles and industry partnerships become more attainable. A deliberate move now may be viable and lead to long-term satisfaction. Case for change Structural forces reshaping medicine, including declining reimbursements, health care system consolidation and administrative responsibilities, are not transient. They are intensifying. The steady increase in burnout and the recognition of misaligned values are stronger predictors of dissatisfaction than income, confirming that physicians who protect their careers effectively take these signals seriously and honestly evaluate how the signals align with their personal vision. When physicians leave, it is rarely because of failure. It is because staying would have required them to become a different doctor than the one they aspired to be. Change, when it is right, is not the end of a

Moving Forward Without Going Back
By Kari McBride “So, when are you going back to work?” I have danced around this question so many times that I think my dance moves now wear a permanent path. It wasn’t that I didn’t want to answer the question; it was that I didn’t know how. I felt embarrassed, guilty, and a little ashamed that I wasn’t working yet. After all, isn’t our value as a person supposed to come from what we do for a living? At least that’s how it often feels in society today. Even after four-and-a-half years of brain injury recovery, new autoimmune diagnoses, one close brush with death, daily chronic pain, and a fight for “normalcy,” I still can’t answer this question. But what I can answer is this: “When am I going to live my life?” And that answer is: Now. I am living my life now. It may be true that I was living this life yesterday, and the day before, and the year before, and so on. But I would argue that it was not the same life. I am not the same person today that I was yesterday. And I am certainly not the same person I was before my injury. My life seems to have been divided into different series: “Before the accident,” and “After the accident.” I can’t say that one is better than the other. The “before” series ends with me as a single mother, newly graduated with a Master of Social Work, employed as a school social worker, and full of energy for all that life had in store. The irony is that the “after” series starts the very next day, but features this girl I don’t recognize. She is living in my body, in my house, with my child. She is no longer working, but instead is on extended medical leave. Her new graduate degree lies off to the side, just another piece of paper. Her days are filled with therapy, appointments, medication, and pain. She is living a life I no longer recognize as my own. “So…when are you going back to work?” Am I going back? What does it even mean to go back? Life didn’t stop just because I was injured. In fact, it’s quite the opposite. In many ways, life seems to have sped up and rushed past, leaving behind only a blur. The job I had at the time is long gone, posted and filled within a few months. My child is four years older and no longer in elementary school. And that fresh degree is covered in as much dust as its accompanying textbooks. Yet somehow, I moved forward without going back. I recently found myself sitting downtown at the state capitol, waiting to meet with my state representative. My stomach was full of knots, and my palms were sweaty. I could feel the early warning signs of a migraine attack and the little daggers piercing my forehead. I had chosen my highland cow tote bag for good luck, and I kept checking to make sure my notes were safely tucked inside. This meeting was important, and nothing could shake my confidence. It had taken years of lived experience, pain, and hard work to find my own value. The moment was now, and I was ready. It was on the car ride home that I realized I may not have gone back to work, but I was working. Just in a different way. I am working to be a bold voice when so many are already talking. I am working in a way that brings meaning to my life. I am working in a way that my body and my brain allow. As it turns out, my social work degree has proved far more valuable in my journey as a patient. I experienced first-hand the value of advocacy, the impact of disability, and the stigma of chronic illness. I fought for my own self-worth and refused to let employment determine my value to society. I am living my life the way I want … the way I can. So perhaps the question isn’t “When are you going back to work?” but rather: “How are you living your life now?” —by Kari McBride Source link
Gut Microbiome and Colorectal Cancer
Nicole Pajer Nicole Pajer is a freelance writer published in The New York Times, Parade, AARP, Woman’s Day, Men’s Journal and beyond. When she’s not writing, she’s checking exotic travel destinations off her bucket list, attempting to wear out her 71-pound Doberman’s boundless energy and teaching people how to properly pronounce her last name (“It’s Pager, just like the beeper!”). Keep up with her adventures on Twitter @NicolePajer. Medically reviewed by Cynthia Sears, M.D. Source link

Are Hypopressives Beneficial for Pelvic Floor Dysfunction?
Estimated reading time: 8 minutes In this article, we will as the question Are hypopressives beneficial for pelvic floor dysfunction? If you are suffering from pelvic floor dysfunction, you may well have heard of Hypopressives; a breathing technique that uses a stomach vacuum to tap into the relationship between the pelvic floor, core and breathing diaphragm. These stomach vacuums are the same as those practiced by yogis for millennia and utilized by bodybuilders since the seventies to enhance breathing, reduce waist size and improve aesthetics. The idea that these stomach vacuums could be beneficial for treating pelvic floor dysfunctions was first suggested in the eighties when Belgian physiotherapist Marcel Caufriez began using hypopressive exercises to improve pelvic floor control in patients. With 1 in 3 women1 suffering pelvic floor dysfunction during her lifetime, finding conservative and easy to follow exercises to improve symptoms and quality of life is critical. So, let’s first explore the exercise before delving into its perceived benefits for those with pelvic floor dysfunction. How to Perform a Hypopressive Exercise (Stomach Vacuum) The hypopressive manoeuvre (also known as an apnea) involves emptying the lungs completely and immediately closing the airways to prevent air reentering the lungs. Following this, the abdominals are relaxed and the ribcage is expanded which creates a stomach vacuum causing the abdominals the be drawn upwards and inwards. The vacuum can also be seen on the back of the body and around the shoulder blades. Follow the steps below to perform the hypopressive manoeuvre which is shown in the animation. Steps to Perform a Hypopressive Apnea Perform three breath cycles where you inhale and exhale. On the third exhalation, empty the lungs fully, this will include contraction of the abs to empty the reserve volume from the lungs. Close your airways to prevent air from reentering the lungs. Take your apnea. To do so, relax the abdominals and expand the ribcage out to the sides in the same motion used when breathing but without taking air in. Hold for a count of 4. Relax the ribcage and abdominals before taking your next inhalation. Animation of a Hyperpressives stomach vacuum Should You Replace Kegels With Hypopressives? For those suffering from a Pelvic Organ Prolapse, the uplifting motion produced when performing an apnea can feel quite relieving on the prolapse, as is my experience with my own rectocele. Of course, feeling some immediate relief doesn’t necessarily mean that there are proven benefits. Marketing of hypopressive training is strong, and some campaigns even suggest using hypopressives as an alternative to Kegel exercises (Traditional Pelvic floor muscle training). In keeping with the usual approach on this website, we will explore the research to see if this makes sense, and to discover the proven benefits of practicing hypopressives. Traditional pelvic floor muscle training (Kegels) as a treatment for incontinence and prolapse is backed by decades of research confirming the benefits. Hypopressives, on the other hand, have only been studied during the last decade. The first study2 into hypopressives compared a group performing Kegels with another performing hypopressives. The conclusion was that hypopressives were less effective than Kegels alone. A subsequent study3 in 2012 had three groups; one performing hypopressives plus Kegels, a second performing Kegels alone and a control group. That study found that both groups performing exercises did better than controls, however; adding hypopressives to Kegels didn’t improve pelvic floor function and those who practiced only Kegels had superior pelvic floor endurance. Another 2012 study4 directly compared a group performing Kegels with another performing hypopressives and found that both groups showed similar improvements. Since those early studies, there have been numerous other studies, none of which have confirmed that you should ditch your pelvic floor exercises in favour of a hypopressive practice, however; through the course of these studies, the true benefit of hypopressives has been revealed. Seated Hypopressive Pose showing the apnea. A Program of Hypopressive Exercises Showed Positive Results in Post-partum Abdominal Diastasis5 The Real Benefits of Hypopressive Exercise If you are suffering from pelvic floor dysfunction, it is very likely that you also have some core weakness. This is where hypopressives can provide benefits. Whereas the early studies into hypopressives did not substantiate the suggestion that they should be used as an alternative to Kegels, they did reveal improvements in the strength of the transverse abdominis (TrA), one of the key core muscles. A 2021 study6 exploring how the abdominal muscles change during hypopressives found that hypopresives significantly increase the thickness of the TrA and internal oblique during the exercise in comparison with the muscles at rest. With that said, you should’t rush to swap your core exercises with hypopressives. A 2020 study7 that looked at the pelvic floor and abdominal muscle response during hypopressives did note that the muscles showed increased activation during the exercises, but not sufficiently to create strength gains. They did, however, suggest it could have an endurance effect. Further studies would be needed to substantiate that hypothesis. Why Practice Hypopressives? So why bother practicing hypopressives if they aren’t going to heal your prolapse or cure your incontinence? I have three reasons why I personally practice hypopressives, and why I included them in some of the breathing modules of my Eight-phase training course. Reason 1 One of the main reasons I like to practice hypopressives is because it relieves the symptoms of my rectocele. I generally only feel symptomatic if I allow myself to get constipated and have to strain to poop. When I get the heavy dragging feeling of the prolapse, I practice my hypopressives and it helps to reduce the symptoms. I also find inversions to be helpful with symptom relief. Reason 2 One of the triggers for the symptoms of prolapse, which is also a cause of leakage during stress incontinence, is increased intraabdominal pressure. When you practice hypopressives, you tap into the relationship between the breathing diaphragm, the core and the pelvic floor. I find that my hypopressive practice helps me to feel and manage this


