Español June is Dysphagia Awareness Month. Eosinophilic esophagitis (EoE) is a condition that causes chronic inflammation in the esophagus. This inflammation results in symptoms like trouble swallowing, chest pain and food impaction (when food gets stuck in the esophagus). While there is no cure for EoE, there are effective treatments to control symptoms and keep the condition in check. Without treatment, EoE typically worsens. EoE is becoming more common, and can affect people of any age. We spoke with Evan S. Dellon, M.D., MPH, gastroenterologist, and professor of medicine and adjunct professor of epidemiology at the University of North Carolina Chapel Hill, to learn more about EoE symptoms, how to get help and treatment options. What symptoms of EoE should prompt you to go to the doctor? In adults and adolescents, the most typical symptom is trouble swallowing or food getting stuck. It’s important to note that food going down slowly or getting stuck is actually abnormal. Many people who ultimately are diagnosed with EoE don’t pay attention to this symptom at first. They might just avoid certain foods or chew more carefully until there’s a major issue. Don’t wait until that happens. Any trouble swallowing or getting food down really should be checked out. Some other gastrointestinal (GI) symptoms, like chest discomfort or heartburn, are also associated with EoE. Other medical conditions can cause food to go down slowly or stick. When these symptoms happen along with asthma or eczema or food allergies, it’s more likely to be a sign of EoE. Children with EoE have totally different symptoms. It could be abdominal pain, vomiting, poor growth, failure to move to different consistencies or food avoidance. Many pediatric GI conditions can cause those symptoms. But they could also be signs of EoE, especially if a child also has eczema, asthma or food allergies as well. If you have EoE, why is getting diagnosed so important? We think that EoE generally starts as allergic inflammation. Over time, if left untreated, that inflammation can progress to scar tissue. Then the esophagus can become narrow and stiff, causing more symptoms and complications like food impaction. Food impaction can lead to a perforation or a rupture of the esophagus, a very severe problem. It doesn’t happen frequently, but these are the complications we worry about. Kids who are affected severely may become malnourished. There’s also an impact on quality of life. Anything that impacts your eating will affect social events, family gatherings, work events and travel and can cause significant anxiety. The symptoms, the impact on quality of life and the potential complications are good reasons to get checked out. How do you get an EoE diagnosis? The diagnostic process comes down to an endoscopy to look into the esophagus. We don’t have any blood tests or other ways to diagnose EoE. The endoscopy is a sedated procedure. A lighted camera goes into the mouth and down into the esophagus and stomach. We look for typical signs of EOE. The esophagus can look swollen. It can be coated with white spots, which is inflammation. There can be scar tissue like rings or strictures. We send a biopsy to a pathologist who examines the allergy cells, which are the eosinophils. If there are enough eosinophils, and we can eliminate other things that might cause them, we can formally diagnose EoE. Why is it important to have continuous care if you have EoE? EoE is a chronic condition that needs to be managed over time. If people are diagnosed but not treated, many will ultimately develop more severe complications. It’s important to have a team in place and be consistent with treatment. There’s a range of severity with the condition. The team will customize the approach for each person’s situation. Someone who has been to the emergency room with an impaction, for example, will be followed much more closely than someone with mild symptoms. Continuous care is different for every person, but it’s very important to have it in place to avoid flare-ups and worsening problems. What types of healthcare providers should be part of your care team if you have EoE? Some people will be followed primarily by GI doctors. Some people will follow primarily with allergists. Some people may follow with both in more of a multidisciplinary fashion. Children may also need feeding therapists and other multidisciplinary providers. We often work with dieticians or nutritionists. How do you manage EoE? There are two major treatment categories: Diet elimination and medication. We think that EoE is a food-triggered condition for most patients. Unlike a typical food allergy, with an immediate reaction, it’s a condition where eating certain foods over a long period of time triggers inflammation. Current allergy tests are not really accurate for EoE, so it’s a little tricky. But we do know the most common food triggers: dairy, wheat, eggs, soy, nuts and seafood. Elimination diets can be used to identify food triggers and remove them from the diet. It’s a good option, but it really depends on the individual patient. Anti-acid medicines such as omeprazole (Prilosec) or lanzoprazole (Prevacid) are often the first medicine we try. Around 30%–40% of people may respond to these simple medicines. Then there’s a topical steroid. We now have an approved medication, budesonide oral suspension (Eohilia), that’s specifically formulated to stick in the esophagus. It can be effective in 50%–60% of people, if not more. Another we use is dupilumab (Dupixent), a systemic medicine. It’s a weekly injection that blocks some of the allergy factors that cause EoE. Typically it’s reserved for people who aren’t responding to other treatments. It might also be used for people being treated for asthma and eczema as well as EoE because dupilumab is approved for all of them. Why is management of EoE a lifelong process? The vast majority of people can get EoE under control, but it is chronic. If people are not treated, they tend to have issues down the road. Not everyone will have complications, but
Why You Should Consider Cycle Syncing Workouts
Gym girlies have to deal with something daunting to the burliest bodybuilders: Our periods. If you feel weaker or more tired at certain times of the month, you’re not alone. Your menstrual cycle affects sleep, mood, bone health, energy, and metabolism, so depending on which stage you’re at in the menstrual cycle, your body may feel up to different tasks. Being in tune with your body and where you’re at in the menstrual cycle can aid in rest and recovery, helping you reach your fitness goals. Here’s how your body changes throughout the menstrual cycle, and why you may want to consider cycle syncing workouts. The Four Phases of Your Menstrual Cycle Your menstrual cycle is driven by two main hormones, progesterone and estrogen, and as levels of these hormones rise and fall in the body, they impact many other processes in your body that can affect exercise. Let’s break down the four phases of your menstrual cycle: The Menses Phase The menses phase begins on the first day of your “period,” aka when you start bleeding. If pregnancy hasn’t occurred, the unfertilized egg is shed, along with the lining of your uterus, through your vagina with waste blood. The Follicular Phase This phase overlaps with the menses phase and ends when you ovulate. Estrogen rises in the body, thickening the uterine lining. Another hormone – literally called follicle-stimulating hormone (FSH) – causes follicles in your ovaries to grow, and one of these follicles will develop into a fully mature egg. Ovulation After an egg is formed, a surge of luteinizing hormone (LH) pushes your ovary to release the egg into the uterus in a process known as ovulation. The Luteal Phase The egg leaves the ovary and starts traveling through your fallopian tubes to your uterus. Progesterone rises in the body to prepare your uterine lining for pregnancy; if pregnancy doesn’t occur, progesterone and estrogen levels drop and your body enters the menses phase again, shedding the thickened uterine lining. Best Exercises for Each Phase One often under-discussed aspect of female training is the importance of pelvic floor strength. A strong pelvic floor functions as the base of the core, manages intra-abdominal pressure, prevents leakage, and supports pelvic organs when performing high-impact activities such as running or lifting. Pelvic floor strength fluctuates as you go through your menstrual cycle, which is why you may struggle to hit new PRs during certain phases after crushing it the week before. Though testosterone is the gym buzz word associated with strength, in people with menstrual cycles, estrogen actually promotes muscle strength, while progesterone relaxes the muscles in preparation for pregnancy and causes your pelvic floor muscles to feel weak. Generally, most people feel weakest during the menstruation phase (days 1-7) when hormones are at their lowest, and strongest during the luteal phase (days 21-28). By cycle syncing workouts, you can take advantage of days where your pelvic floor muscles are strongest and energy levels are highest. Understanding why you don’t feel as up to intense training during the luteal phase can (weaker pelvic floor muscles mean less stability!) can be helpful for mitigating overtraining or injury. Menstrual Phase (Days 1-5) Energy levels are typically low during the menstrual phase. A dip in estrogen and progesterone can cause your pelvic floor muscles to weaken, and you may feel fatigued. If you feel tired during this phase, don’t push it; take a rest day, or stick with light activities like stretching or walking that get the blood flowing without compounding fatigue. If you have a heavy menstrual flow, make sure you’re eating enough iron to compensate for blood loss. Follicular Phase (Days 6-13) You’ll typically feel better during this phase as energy levels increase with estrogen levels, making it a good time to hit that Crossfit class or tack on some hill springs. Your pelvic floor should be feeling good, as rising estrogen levels enhance strength, muscle tone, and coordination. Ovulation Phase (Days 14-17) This is the time to try for a new deadlift PR or record swim time – estrogen and testosterone levels peak in the body during ovulation, heightening muscle tone and coordination. Luteal Phase (Days 18-28) Rising progesterone levels during the luteal phase can start slowing you down, especially later on in the cycle approaching your period. This is why you may feel extra fatigued or crampy the days right before your period starts. If you tend to feel especially tired towards the end of your cycle, try to focus on activities involving more pelvic floor strength like high-intensity strength training or cardio in the earlier days of the luteal phase, before progesterone levels peak. You can plan your lower-intensity Pilates or yoga classes for the end of the luteal phase. Every Body Is Different While hormonal fluctuations during your menstrual cycle can influence training and exercise, it’s important to remember there’s no way to pinpoint your exact hormone levels. Tracking your period and knowing what stage you’re probably at is a general guide, and the most important thing is to listen to your body and how it feels. There’s no rule saying everyone with a cycle absolutely SHOULD lift hard during the luteal phase, or that you have to take days off during the menstrual phase. Many of us already find it difficult to fit exercise into our busy schedules without having to organize around our menstrual cycles. Unfortunately, people with cycles are underrepresented in sports and exercise studies, where the majority of the research focuses on male participants or doesn’t account for menstrual cycles. Cycle syncing isn’t an exact science, but understanding how your menstrual cycle can impact exercise performance should help you give yourself a little grace on the days you mysteriously can’t lift as well as previously, or to explain why certain times of the month you feel like superwoman. Source link
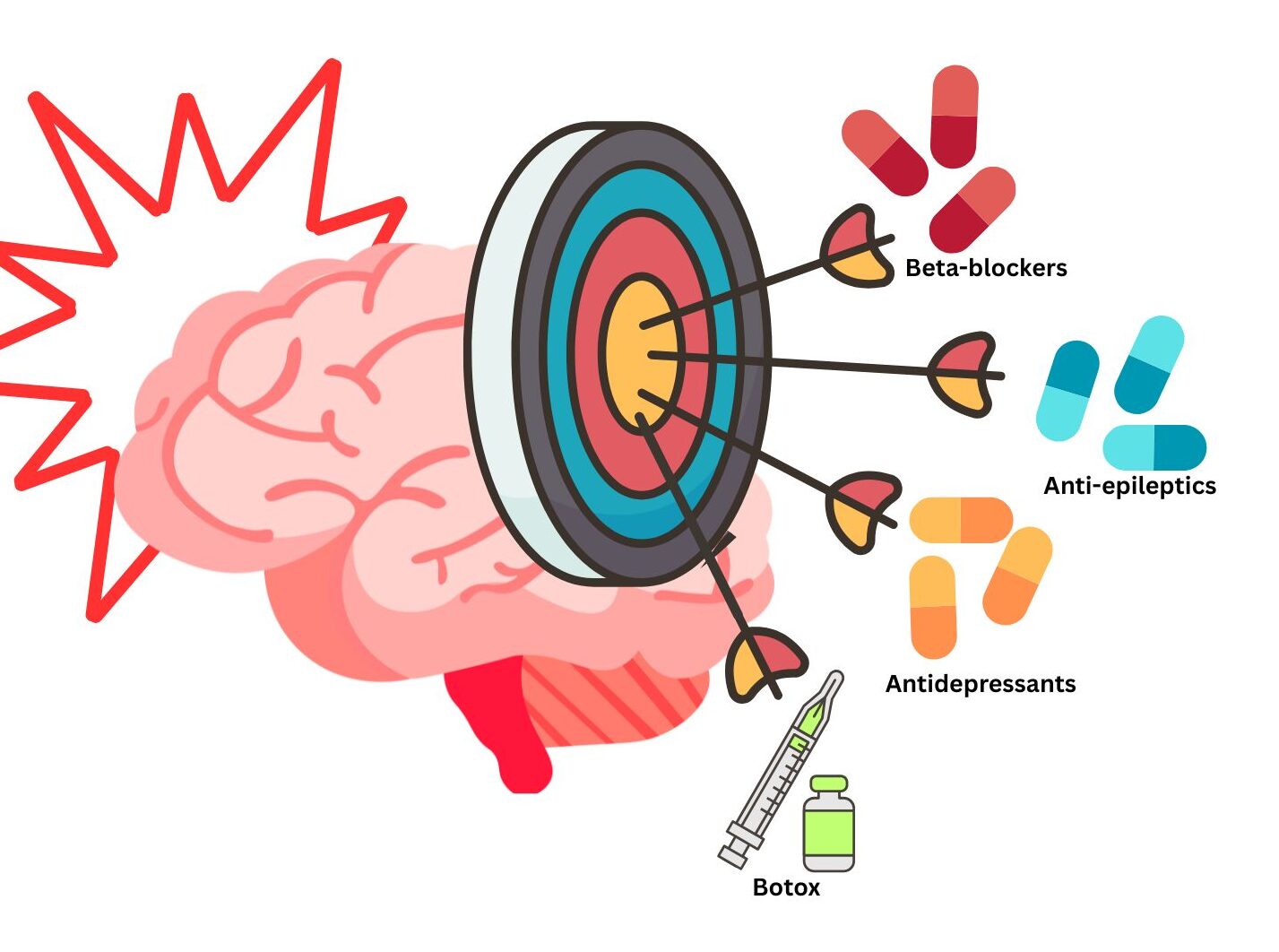
From Botox to beta blockers: how medications developed for other health conditions are used in migraine
How Repurposed Medications Work in Migraine Many older migraine medications, especially those used as preventives, were not originally developed to treat migraine. In reality, several commonly used migraine preventives were actually developed to treat a variety of conditions from high blood pressure to epilepsy. However, coincidentally, people taking these drugs started to report that their migraine attacks were getting better leading researchers to explore their use as migraine treatments. This might seem surprising, but when we look at the science, migraine and these conditions share some overlapping biology, including changes in the way our neurons (brain cells) communicate and the chemicals they release to do so. One example of this is a brain chemical called serotonin, which is involved in migraine and mood disorders, and therefore a medication that could stabilise serotonin has the potential to work in both. These repurposed medications aim to reduce attack frequency and severity (preventive medications) rather than treat an existing attack (acute medications). Examples of repurposed migraine medications include: Mignon Van der Watt, Canva 2026 Beta blockers (e.g. propranolol) What was it originally used for? Medications like propranolol were originally designed to treat heart conditions and high blood pressure. They primarily work by blocking the activity of stress hormones like adrenaline and noradrenaline that underlie the ‘fight or flight’ response, leading to a slower heart rate and lowered blood pressure. How might they work to help prevent migraine attacks? Although migraine biology is complex, researchers believe the beta blockers’ ability to calm down the body’s stress response may help it to reduce the sensitivity of migraine-related brain pathways and dampen some of the abnormal nerve signalling involved in attacks, potentially reducing their frequency. They may also influence chemicals involved in pain and inflammation, including CGRP. Beta blockers are considered a first-line preventive treatment for migraine and are often a first choice for people who also have conditions like high blood pressure or anxiety. Anti-epileptic medications (e.g. topiramate) What was it originally used for? Medications like topiramate were originally designed to treat epilepsy and seizures. These medications prevent seizures by rebalancing the excitability of neurons in the brain. How might it work to help prevent migraine attacks? Migraine and epilepsy both include changes in the electrical activity of neurons in the brain. Because both conditions share some of the same underlying mechanisms, anti-epileptic medications can be repurposed to help stabilise overactive brain activity in migraine. It is important to note that women who are considering planning a pregnancy should avoid taking anti-epileptic medications, like topiramate, as it may cause harm to an unborn baby. Antidepressants (e.g. amitriptyline) What was it originally used for? Medications like amitriptyline were originally designed to treat depression. Antidepressants work by altering brain chemicals such as serotonin and noradrenaline. How might it work to help prevent migraine attacks? Both serotonin and noradrenaline play a role in migraine biology by influencing pain pathways, mood changes and sleep. At lower doses, antidepressants may alter these chemicals to help the brain process pain differently and improve sleep, which can help reduce migraine frequency. Botox What was it originally used for? While we may now associate Botox with cosmetic procedures, it was originally used to treat eye muscle disorders. It works by temporarily preventing muscles from contracting through blocking the release of a brain chemical, acetylcholine, that signals muscles to move. How might it work to help prevent migraine attacks? Botox is a treatment that can be used in people living with chronic migraine. It works by calming overactive nerves and by blocking pain signals. In addition to reducing the frequency of migraine attacks, it can also reduce how severe a migraine attack is. How repurposed drugs expand migraine care We know that migraine treatment is highly individual. What works well for one person may not work well for another, which often leads people to try several options before finding the right fit. Drug repurposing helps expand the treatment options available. Using existing medications that have been shown to be effective for migraine can save time and cost, as researchers often already understand their safety profiles, allowing access to treatments to be accelerated. Although these medications are established, they can still cause side effects and should be prescribed and monitored appropriately. Not every medication works for every person, and treatment decisions should always be made with a healthcare professional. Not only can drug repurposing increase the number of medications available for migraine management, but they can also teach researchers more about migraine biology itself. While this approach has worked and we now also have targeted preventive therapies, it’s clear that a medication doesn’t need to be designed specifically for migraine to make a real difference to people living with it. You can learn more about these preventive medications for migraine here. Source link

AMA calls for AI regulations in clinics, insurance
Add topic to email alerts Receive an email when new articles are posted on Please provide your email address to receive an email when new articles are posted on . “ data-action=”subscribe”> Subscribe We were unable to process your request. Please try again later. If you continue to have this issue please contact customerservice@slackinc.com. Back to Healio Key takeaways: At its annual meeting, the AMA adopted new policies stressing the need for physician oversight. They also advocate for more transparency when AI is used in both clinical and in health insurance decision-making. The AMA adopted new AI policies in a bid to ensure that the technology supports evidence-based medicine, bolsters patient care and serves under a physician’s oversight, instead of replacing their discernment. According to an AMA press release, AI technologies could help with efficiency and synthesizing information, but there are still important concerns for bias, long-term impact on both physicians and patient outcomes, explainability and transparency. At its annual House of Delegates meeting, the AMA adopted new AI-related policies. Image: Adobe Stock These new policies, which address AI’s growing popularity in both the clinical and health insurance decision-making realms, emphasize that AI should only be used as an assistive tool, rather than “an autonomous decision-maker,” according to the release. The policies also call for accountability, transparency and oversight from physicians every time AI is used in patient care. “AI has enormous potential in health care, but it cannot replace physician judgment,” John Whyte, MD, MPH, CEO of the AMA, said in the release. “Patients deserve care decisions that are informed by the latest medical evidence and guided by a physician who understands their individual needs. Whether AI is helping a physician make a clinical decision or assisting with an insurance review, there must always be transparency, accountability and meaningful physician oversight. Technology should support better care — not stand between patients and the care they need.” The AMA has said it will work with key stakeholders — including regulators, medical specialty societies and AI developers — to create standards for evidence transparency, evaluation, attribution, validation and explainability in systems that support clinical decision-making. This is in the hope of ensuring AI tools “reflect the principles of evidence-based medicine and provide physicians with information they can understand, evaluate and trust,” according to the release. Another AMA policy calls for regulations to guarantee that health coverage decisions — which are increasingly based on AI, according to the release — are reviewed by physicians in appropriate fields with a foundation of evidence-based, up-to-date medical information. The policy additionally called for safeguards requiring AI technologies be integrated into a physician-led process and increased transparency when AI is involved in prior authorization decisions, including the disclosure of any guidelines, data sources or clinical logic used in adverse decisions. In this vein, the AMA is advocating for regular audits of clinical review tools driven by AI to help strengthen accountability. That also includes audits triggered by “significant changes to” training data, clinical guidelines or AI models themselves, “as well as comprehensive annual reviews to ensure continued alignment with standards of care,” according to the release. “When health plans use AI-driven tools to deny or delay care without explaining how those decisions were reached, physicians and patients are left in the dark,” Whyte said in the release. “AI should never function as an unaccountable black box. Health plans must be transparent about how these tools work, what evidence and data sources they rely on, and whether a qualified physician reviewed the decision.” Perspective Back to Top The idea that AI should “support, not replace” physician judgment is not controversial. It’s obvious. The real issue is that, across health systems today, we are already drifting in the opposite direction — quietly, incrementally and often without enough oversight. AI tools are being embedded into workflows, influencing decisions and shaping clinical behavior faster than governance models can keep up. How many physicians are actually aware that they are using AI? The greatest risk is not that AI will replace physicians overnight. It’s that it will subtly erode clinical judgment through automation bias, opaque recommendations and overreliance on systems that clinicians neither fully understand nor control. In that sense, the danger is not disruption, it’s complacency. What the AMA policy stops short of saying explicitly is this: physician oversight alone is not enough. Oversight without infrastructure, governance and accountability is performative. Health systems need enterprise-level AI operating models — clear standards for validation, monitoring and lifecycle management — because fragmented, point-solution AI adoption is already creating measurable clinical and operational risk. Deepti Pandita, MD, FACP, FAMIA University of California Irvine Health Disclosures: Pandita reports no relevant financial disclosures. Sources/Disclosures Source: Press Release Disclosures: Whyte reports being CEO of the AMA. Ask a clinical question and tap into Healio AI’s knowledge base. PubMed, enrolling/recruiting trials, guidelines Clinical Guidance, Healio CME, FDA news Healio’s exclusive daily news coverage of clinical data Learn more Add topic to email alerts Receive an email when new articles are posted on Please provide your email address to receive an email when new articles are posted on . “ data-action=”subscribe”> Subscribe We were unable to process your request. Please try again later. If you continue to have this issue please contact customerservice@slackinc.com. Back to Healio Source link

How Long Does an Epidural Steroid Injection Last?
If your doctor has recommended an epidural steroid injection to treat your back pain or another chronic pain condition, you probably have questions — especially about how long the relief will actually last. The honest answer is that it depends on the person, but understanding what affects duration can help you set realistic expectations and get the most out of your treatment. What Is an Epidural Steroid Injection? An epidural steroid injection (ESI) is a minimally invasive procedure used to relieve pain caused by inflamed spinal nerves. A physician injects a corticosteroid — sometimes combined with a local anesthetic — directly into the epidural space of the spine, which is the area surrounding the spinal cord and nerve roots. These injections are commonly used to treat conditions like herniated discs, spinal stenosis, degenerative disc disease, and sciatica. They’re one of the most widely used pain injections for back problems because they can reduce inflammation at the source, rather than just masking discomfort systemically the way oral medications do. How Long Does an Epidural Steroid Injection Last? This is the question most patients ask first, and the answer varies more than people expect. For some patients, relief lasts a few weeks. For others, a single injection can provide significant improvement for three to six months — or even longer. A smaller group of patients experience only minimal or temporary relief. Several factors influence how long the effects last: The underlying condition. Acute flare-ups of a chronic condition tend to respond better than long-standing, severe degeneration. How inflamed the nerve root is. The more targeted the inflammation, the more precisely the steroid can work. Your overall health. Factors like weight, activity level, and whether you smoke can all affect outcomes. The type and location of the injection. There are different approaches — interlaminar, transforaminal, and caudal — and the right technique depends on your specific anatomy and diagnosis. It’s also worth noting that the local anesthetic included in many injections provides immediate but short-lived relief — typically a few hours — while the steroid takes a few days to reach its full anti-inflammatory effect. So don’t be discouraged if you don’t feel dramatically better the same day. How Many Injections Will I Need? Most physicians recommend a series of up to three epidural steroid injections per year at any given spinal level. This isn’t arbitrary — repeated steroid use can have side effects, including thinning of nearby tissue or temporary changes in blood sugar levels. Some patients need only one injection per treatment cycle. Others benefit from two or three spaced a few weeks apart, especially when the first injection provides partial relief. Your pain specialist will assess your response after the first injection before recommending additional ones. The goal isn’t to keep injecting indefinitely. Epidural steroid injections work best as part of a broader pain management plan that may include physical therapy, lifestyle changes, and other treatments. What to Expect After the Injection Most patients go home the same day and can resume light activity within 24 hours. Some soreness at the injection site is normal and usually resolves within a day or two. Keep a symptom journal after your injection. Note when you start to feel relief, how significant it is, and how long it lasts. This information is incredibly useful for your care team when deciding whether to repeat the injection or explore other options. You should avoid strenuous activity, driving (on injection day), and submerging in water like pools or hot tubs for at least 24 hours after the procedure. Your provider will give you specific post-procedure instructions based on your situation. Are Epidural Steroid Injections Right for You? Epidural steroid injections are most effective for pain that has a clear inflammatory component — particularly radiating leg or arm pain caused by nerve compression. They tend to be less effective for purely mechanical back pain without nerve involvement. They’re not a permanent cure, and they won’t reverse structural damage like a severely collapsed disc. But for many patients dealing with injections for chronic pain management, ESIs offer a meaningful window of relief that allows them to engage more fully in physical therapy, return to work, or simply get back to daily life. Your pain specialist will review your imaging, medical history, and symptoms to determine whether this approach makes sense — and if so, which injection technique is most appropriate for you. Frequently Asked Questions How quickly does an epidural steroid injection start working? The local anesthetic may provide same-day relief, but the steroid component typically takes 3–5 days to reduce inflammation. Most patients notice meaningful improvement within one week. Can I get an epidural steroid injection if I have diabetes? Yes, but with caution. Corticosteroids can temporarily elevate blood sugar, so your care team will need to monitor you closely. Always disclose your full medical history before the procedure. Is the injection painful? Most patients report mild pressure rather than significant pain. A local anesthetic is used to numb the skin and underlying tissue before the injection, and many providers offer light sedation for anxious patients. How often can I get epidural steroid injections? Generally, physicians limit injections to three per year at a single spinal level to minimize steroid-related side effects. The timing between injections typically depends on your response to the previous one. What if the injection doesn’t work? If you receive little to no benefit from an ESI, that’s valuable diagnostic information. Your pain specialist may recommend a different injection approach, additional imaging, or an alternative treatment pathway. Taking the Next Step Toward Relief Living with back pain or chronic pain is exhausting, and it’s easy to feel like you’ve run out of options. Epidural steroid injections aren’t a cure-all, but for the right patient, they can be a genuine turning point — one that creates enough relief to move forward with therapy, regain function, and improve quality of life. If you’re weighing your options, the best next step is a conversation with

My Chronic Hives Kept Coming Back
Español As told to Erica Rimlinger The hives first appeared when I was in my early 20s, following a trip to the laundromat. Putting on my newly clean clothes, a rash perfectly outlining the shape of my bra and underwear formed. Shocked and incredibly itchy, I called my mom, who guessed I used too much detergent in my laundry or was having an allergic reaction. She recommended an antihistamine, which didn’t even take the edge off the never-ending itch. Unable to sit down or tolerate clothing touching my angry, red welts, I called the Ask-a-Nurse hotline my health insurance required. After an hour on hold, I was cleared to go to their urgent care. There, a doctor gave me a steroid shot and wrote me a prescription for several days of steroid pills. He told me to stay on an antihistamine and advised against using that detergent brand again. The angry, red hives quickly cooled to pink, calmer ones, then, nearly a week later, disappeared. I thought this episode was a learning experience and that it was over. But it wasn’t over: The hives returned. Each time, my healthcare providers and I assumed some unknown allergen had irritated me. I’d get a course of steroids, keep taking antihistamines and the hives would disappear like magic over the next week. I didn’t care about any long-term side effects of taking steroids: I just needed them to work when I needed them. I kept detailed notes on what I ate and used on or near my skin. I saw an allergist, who couldn’t find a culprit that was causing the outbreaks. In my 20s and 30s, the outbreaks were relatively short, but I’d have to miss life for a week while I dealt with them. The itch was too intense to allow me to focus on anything for very long, and no cream, pill or treatment provided enough relief. In my 40s, the hives were staying longer and not responding quickly to the steroids or multiple antihistamines. By then, when the outbreaks lasted well over a week and felt unmanageable, I was desperate for relief. If you’re imagining hives as a collection of small, red, itchy bumps like mosquito bites, you’re not quite getting the full sensory experience. My hives erupted in painful swells that couldn’t be touched without angering my body and making the itch even worse. It was as if someone shaved off all my skin with a razor and covered me with wool. During my flares, a light scratch of the fingernail along my skin would turn the line into hives. I could write my name in hives on my skin, a phenomenon called dermatographism. In 2019 I had a hive outbreak that lasted months, meaning my hives met the definition of “chronic.” As I had with shorter outbreaks, I found it nearly impossible to work, sit, function or do simple activities like bathing. I had hives every day and didn’t know which days they might be more severe or where the swelling and itching would move to next. The painful itch was oppressive — and nothing relieved it. During flares, I continued to document all the details of my life, looking for any reason for the outbreak’s appearance, disappearance, worsening or relief. I couldn’t find a pattern, an allergen or any clue why this was happening. During my last flare, I also couldn’t find any form of relief that worked anymore. There are many myths about chronic hives, and one is that simply reducing stress eliminates outbreaks. As a woman experiencing a chronic illness, I found medical staff commonly telling me if I would just be calmer, I wouldn’t be sick. But, my regular notetaking about the circumstances surrounding my outbreaks showed me they were not caused by my emotions. It felt dismissive for people to imply I could control the extreme physical reaction my body was having by simply not being stressed — as if that were even possible. CSU on Kristen’s legs The first week of the 2019 outbreak was the worst agony I’d ever experienced, then the outbreak lost predictability entirely. I could not sit still given how severe the itching was. It prevented me from sleeping, working, being with friends and family, and doing basic activities. After a few days, things improved, but the hives were still present every day: first for weeks, and then months. A while back, I’d been diagnosed with an autoimmune disorder called Graves’ disease. I wondered if my hives could be related. After some research and consulting with my immunologist, I learned about chronic urticaria (CU), or chronic hives. In most people with the condition, its cause is never identified, which is called chronic spontaneous urticaria (CSU) — but the outbreaks are strongly linked to autoimmune issues. I was taking steroids and quadruple doses of antihistamines, and they provided no long-term relief. I finally found an allergist/immunologist who knew that CSU is almost never an allergic reaction — despite common misconceptions. She knew what to do next and that gave me great hope. I continued taking antihistamines and started a treatment that required a shot in the back of each arm each month. By month three, I hadn’t seen improvement. I called a friend who is a pharmacist and asked, “Is this going to be forever? Why can’t I get rid of these?” The friend contacted a trusted colleague in the field who told me to stick with it, so I did. Almost like clockwork, by month six, the hives were completely gone. I could cry just thinking about it today. What an incredible relief. Since that time, I have not had an outbreak. While I’ve had an occasional, isolated hive, I’ve had no flare-ups since. I didn’t intend to become an advocate for people with chronic hives, but I was working for a global patient advocacy organization that included CU in its scope of work. When I mentioned to my CEO that I was a CU patient

Natalie Morales on Alzheimer’s and Caregiving
CBS correspondent Natalie Morales is 54, the same age her mother-in-law was when she received a devastating Alzheimer’s diagnosis. So when Morales experienced a memory lapse while on a recent work trip, she couldn’t help but fear the worst. “I’m very well aware of when I have a memory lapse, whenever there’s a word I can’t think of,” Morales told USA Today in an interview this week. “Or if, you know, I know this person but… I can’t think of their name.” On her trip, Morales forgot her hotel room number, spending minutes on the wrong floor tapping her key card against doors. “Oh my gosh,” she remembered thinking. “Either I’m overworking, or I don’t know what’s going on. Maybe I’m having perimenopause brain.” Of course, the thought of dementia also ran through her mind. Her mother-in-law, Kay Rhodes, died in 2014 after living with Alzheimer’s for years. Related story Olivia Munn Describes ‘Surreal’ Breast Cancer Diagnosis: ‘I’d Seen This in Movies’ Morales doesn’t have dementia, but fearing it is understandable — once we get to a certain age, it’s hard not to. That’s especially true when it’s impacted your loved ones. “I think she was always a little bit afraid of getting that diagnosis,” Morales said of her mother-in-law. “And there was a little bit of that denial, although I think she knew better than anyone what she was feeling.” The first signs, Morales remembers, were her mother-in-law having trouble completing tasks and repeating herself while speaking, along with anxiety and paranoia. Rhodes’s struggle with Alzheimer’s also impacted the rest of the family. Rhodes’s husband was her primary caregiver and Morales says he felt the impact physically, emotionally, and financially. “With a lot of caregivers, you know, the more they invest in someone else and in that care, they lose themselves in that,” Morales reflects. Now that Morales herself has some of those same Alzheimer’s fears, she’s both accepting and optimistic about the future. “We are at that age where these are things that we have to talk about and think about a lot more,” she said. But thanks to medical advancements, there are now more treatments than ever for people with dementia, including new medicines, better testing, and drugs that stop Alzheimer’s triggers. “The outlook,” Morales agrees, “is so much more positive now.” Source link
A Visit to Fukuda Lab at Yokohama National
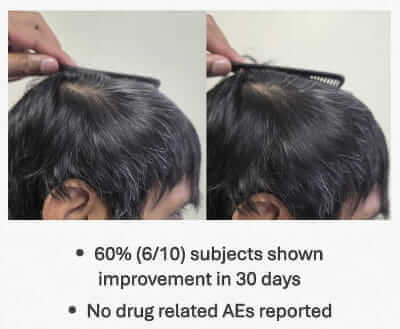
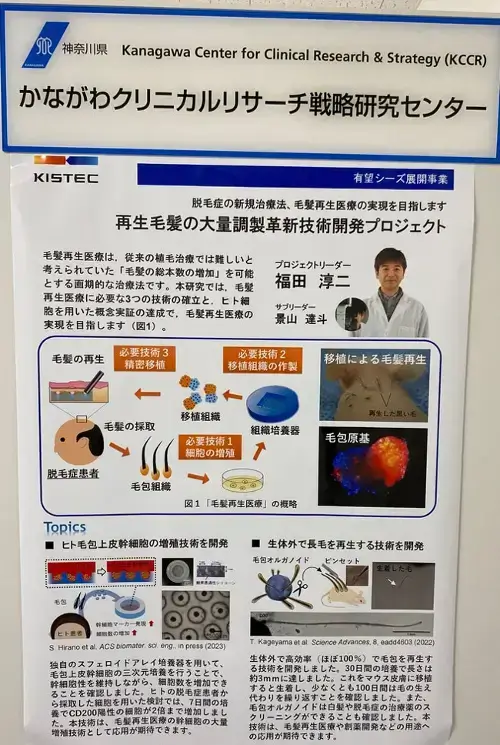
This post was originally written in 2024. I have added new updates from 2025 and 2026 at the bottom. I have extensively covered the work of the esteemed Japanese hair loss researcher Dr. Junji Fukuda for over ten years. Among the posts that I have written in relation to his team’s work at Fukuda Lab include the following: February 21, 2024 A Visit to Fukuda Lab at Yokohama National Reader “Theo” just sent me a link to a very interesting diary of a hair transplant surgeon from Japan who just visited the Fukuda Lab. Note that while Dr. Fukuda is based at Yokohama National University, the research seems to be taking place at Kanagawa Life Innovation Center (per the above link). One of the images also mentions the Kanagawa Center for Clinical Research & Strategy (KCCR). Yokohama is the second largest city in Japan and is the capital of Kanagawa Prefecture. Check out this PDF of the regenerative medicine sector at Kanagawa Prefecture. From this visit and summary, I learn some very interesting things. There are three distinct methods in which Dr. Fukuda is pursuing hair regeneration. I mentioned them in my past lengthy post too, but now we have more clarity. 1) Dermal Papilla Cell Transplantation “Dermal papilla cell transplantation is about to begin in Japan.“ Transplantation of dermal papilla cells (via stratified culture). I assume that the “stratified cuture” in the translation means 3D culturing. Dr. Fukuda mentions that Shiseido already conducted a clinical trial using 2D culturing. In this method, cells are are lined up on a flat surface when culturing, but it only resulted in a 5% increase in hair volume. The 3D method will likely be superior and the clinical trials are about to finally begin! It is hoped to be “put into practical use within five years”. 2) Transplantation of Hair Follicle Primordium “I think this will take some time.” The creation of hair follicle primordia means generating hair from scratch. i.e., hair multiplication. I previously discussed the Yokohama team’s process of achieving this via increasing and mixing epithelial cells and mesenchymal cells. These then form “hair follicle primordia“ that are transplanted to the same donor’s scalp in order to regenerate hair in thinning regions of the scalp. Per the latest feedback from Dr. Fukuda, while this process has already been proven by them in mice, human hair is a different animal. Once the primordium tissue is transplanted to human heads, the direction and length grow haphazardly. He thinks that this will take some time. 3) Transplantation of Regenerated Hair Follicles in Vitro (Organoids) “It will likely take more than 10 years before it can be used in humans.” The final method is in vitro regenerated hair follicle transplantation (also called organoid). In this process, hair follicles are regenerated outside the body, lengthened by almost 100%, and then transplanted into the scalp. Per Dr. Fukuda, it will likely take more than 10 years before it can be used in humans. Other Notes In March 2023, Dr. Fukuda and his Yokohama team published an important hair regeneration related study. They made an improvement in the expansion of hair follicle stem cells (HFSCs) and dermal papilla cells via the use of a newly designed microwell array device. Fukuda Lab’s hair research summary poster. Source:Naohiro Uchida, Director of Almo Plastic Clinic Hair Transplantation. Update: April 18, 2024 New Junji Fukuda interview given to Tokyo Television. Someone please translate it into English if you know Japanese. Not yet on YouTube. Junji Fukuda TV Interview. Update: June 15, 2025 Yet Another Visit to Fukuda Lab Yet again, Tokyo TV visited world renowned hair loss researcher Dr. Junji Fukuda at Yokahama National University. A Japanese reader posted a link to the full video in the comments, but it did not load for me. However, I managed to find two of the segments on YouTube. You can turn on English captions in the videos. The Japanese viewer comments underneath the first video are funny. Update: June 12, 2026 A number of new updates in recent months. In December 2025, Dr. Fukuda gave an interesting interview. He said that his team’s initial goal is to popularize hair regeneration therapy, thereby establishing the necessary infrastructure (such as cell processing facilities). In the future, they aim to expand this technology to regenerative medicine for various organs, in particular, the liver. Quote: “Hair is naturally formed by two types of cells (epithelial cells and mesenchymal cells) exchanging information with each other. We are challenging ourselves to unravel the mechanism of this “interaction” and completely reproduce it in a culture dish. In fact, most of the organs in our bodies are formed by the interaction of these two types of cells.” Of note, Dr. Fukuda is described as the President and CEO of TrichoSeeds, a company he co-founded several years ago. He also continues to work at Yokohama National University via Fukuda Lab as a professor and researcher. In March 2026, Dr. Fukuda co-authored a paper on the potential of employing hiPSC-derived ectodermal precursor cells in hair follicle organoid cultures in hair regenerative medicine. In April 2026, it seems like the Fukuda Lab got some funding from Beyondge Capital (Japan). Also in April 2026, Dr. Fukuda gave a presentation titled: “Treatment of male pattern baldness using microRNA produced by human papilla cells in stratified culture.” In April, Dr. Fukuda and his team authored yet another paper. They discuss their findings about the correlation between reduced CD200 expression and increased hair regenerative capability of cultured hair follicle bulge cells. Quote: “Our study refines the functional interpretation of CD200-defined bulge heterogeneity and provides insights for optimizing human bulge cell-based approaches to hair follicle regeneration.“ Source link
New tool launched to help improve headache and migraine care
This week, The Migraine Trust and The Neurological Alliance launched Improving headache and migraine care together: A tool for NHS professionals & providers. The new tool is designed to help NHS commissioners, providers and professionals to plan, design and improve local services for people of all ages affected by headache and migraine. It identifies and signposts to the best available resources and provides a framework for local service transformation. Developed by The Migraine Trust and the Neurological Alliance with support from people living with migraine, health professionals, service managers at Integrated Care Boards (ICBs) and NHS provider representatives from across England, the tool is focused on care pathways that can be delivered in the community with key stakeholders, partners and services. Rob Music, Chief Executive of The Migraine Trust, said: “We know that many people with migraine find it challenging to access the care they need or deserve. At the same time, we recognise it can be challenging as a commissioner, provider or healthcare professional looking to improve services to know where to start. The launch of this tool marks an important step in moving toward consistent, high-quality care for people living with migraine.” Georgina Carr, Chief Executive of Neurological Alliance, said: “This tool offers a blueprint for best practice headache and migraine care in local settings and supports the NHS 10 Year Plan’s ambition to move care from hospitals to communities. We hope it will empower local healthcare leaders to improve headache and migraine services, which will not only improve patient outcomes but also reduce pressure on secondary care services.” Improving headache and migraine care together: A tool for NHS professionals & providers is endorsed by the British Association for the Study of Headache (BASH), Association of British Neurologists (ABN) and British Paediatric Neurology Association (BPNA). Alex Sinclair, Chair of BASH, said: “BASH welcomes this practical, evidence-informed tool, which brings together the key resources needed to improve headache and migraine care across the NHS. By supporting joined-up pathways, strengthening primary and community management, and enabling timely access to specialist expertise, it represents an important step towards more consistent, high-quality care for people affected by headache disorders.” Dr Rachael Kilner, Clinical Advisor on the project, GP with extended role headache King’s College Hospital, St Thomas’ Hospital and Bromley GP Alliance community headache clinic, said: “Headache disorders represent one of the largest opportunities to improve neurological care across the NHS. Too many people are still experiencing avoidable delays, unnecessary referrals and fragmented pathways. This tool brings together the evidence, clinical guidance and practical resources needed to support more consistent, joined-up care across primary, community and specialist services.” Dr Kay Kennis, Clinical Advisor on the project, GP with extended role in headache, Bradford Community Neurology Service, said: “For many people living with migraine, the difference between good and poor care comes down to whether they can access the right support at the right time. Strengthening headache care in the community has the potential to improve outcomes for patients while reducing avoidable demand on hospitals. This tool supports services to make those changes using evidence-based approaches.” The Migraine Trust is committed to improving care, support and awareness for people with migraine. You can stay up to date with our work here and by signing up to our ebulletin. Financial support for this project has been provided as a Quality Improvement Grant from Pfizer International LLC. Editorial control rests with The Migraine Trust and the Neurological Alliance. Source link
Ambient AI in the exam room: Friend or foe for physicians?
June 12, 2026 11 min read Add topic to email alerts Receive an email when new articles are posted on Please provide your email address to receive an email when new articles are posted on . “ data-action=”subscribe”> Subscribe We were unable to process your request. Please try again later. If you continue to have this issue please contact customerservice@slackinc.com. Back to Healio As the presence of ambient AI scribes to record clinical encounters in the exam room grows increasingly common, experts continue to debate over whether this new technology will ultimately be a friend or foe to physicians. “Ambient AI has the potential to bring about significant changes in what has become the elephant in the room for many physicians: the electronic health record,” Leonard H. Calabrese, DO, chief medical editor of Healio Rheumatology, professor of medicine at the Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, and RJ Fasenmyer chair of clinical immunology at the Cleveland Clinic, said in an interview. Image: Allan Gibofsky, MD, JD, MACR, FACP, FCLM For example, ambient AI can listen to clinical encounters and minimize the time physicians spend on electronic health records, which experts have long cited as a source of bureaucracy-related burnout. However, whether those changes are immediate or universally positive remains to be seen, according to Kenneth G. Saag, MD, MSc, professor of medicine in the division of clinical immunology and rheumatology at the University of Alabama, Birmingham. Kenneth G. Saag “Ambient AI has the potential to alleviate a pretty major challenge, which is that most of the clinical encounter is spent typing,” he said. “But we have to consider whether the AI scribe is capturing salient details and weeding out the chatter.” According to Saag, an ambient AI tool could, in a perfect world, do exactly that and potentially bring back the kinds of doctor-patient encounters he recalls from a generation ago. “It can allow us to look the patient in the eye and return to the interpersonal nature of a doctor visit,” he said. “The hope is that it is not creating more work by requiring a lot of editing.” For Allan Gibofsky, MD, JD, MACR, FACP, FCLM, professor of medicine at Weill Cornell Medicine, and attending rheumatologist and co-director of the Clinic for Inflammatory Arthritis and Biologic Therapy at the Hospital for Special Surgery, the risk for introducing errors into the medical record should be top of mind for any physician. “As with any new technology, we have to temper our enthusiasm for its utilization with caution of how it is going to be utilized,” he said. “For example, what does it mean to use this tool without appropriate professional oversight? Medical records are eternal. If there is an error in a patient’s chart, it gets carried forward and attempts to correct it are, at best, problematic. It is important that the same is not true for the documentation by AI scribes.” Another potential concern is that employers may see the time-saving nature of these products and adjust employee expectations accordingly, said Grace C. Wright, MD, PhD, of Grace C. Wright MD PC. Grace C. Wright “Time is money, and if AI allows you to see patients more efficiently in less time, the patient load may be increased,” she told Healio. “I would prefer to have more issues dealt with in the clinical encounters, such as mental health, life impact and social connectedness, instead of just adding more patients. Undoubtedly, our patients would become healthier if we could spend the extra time managing their overall health.” Additional concerns over the use of ambient AI in the exam room involve potential threats to patient privacy, and the question of when and how to acquire patient consent to use such technologies. However, if these impediments can ever be overcome, the technology could fundamentally alter the way medicine is practiced, according to experts. ‘Redesign the choreography’ In a 2025 paper published in JAMA Network Open, Olson and colleagues surveyed 451 physicians who used an AI scribe in the clinic for 30 days to determine whether use of the technology saved them time and reduced burnout. Among the 272 physicians from multiple specialties who completed both the pre- and post-intervention surveys, results at 30 days showed that the proportion of respondents who reported experiencing burnout decreased significantly from 51.9% to 38.8% (OR = 0.26; 95% CI, 0.13-0.54). Further results showed that use of an ambient AI scribe was associated with significant improvements on a 10-point scale in burnout (mean difference, 0.47 points; standard error, 0.12), note-related cognitive task load (mean difference, 2.64 points; standard error, 0.13), ability to provide undivided attention (mean difference, 2.05 points; standard error, 0.18), patient understandability of their care plans from reading the notes (mean difference, 0.44 points; standard error, 0.17), and time spent documenting after hours (mean difference, 0.90 hours; standard error, 0.19). “This multicenter quality improvement study found that use of an ambient AI scribe platform was associated with a significant reduction in burnout, cognitive task load, and time spent documenting, as well as the perception that it could improve patient access to care and increase attention on patient concerns in an ambulatory environment,” the researchers wrote. Although Calabrese said he is encouraged by such findings, he noted that simply having the tool is insufficient to reshape the clinical experience. Leonard H. Calabrese “This technology has the potential to redesign the choreography of the practitioner-patient dyad that has been with us for 20 years since we have been using the laptop and the EHR,” he said. “However, I have strong doubts that everyone who starts using ambient AI will be on a trajectory to optimize their practitioner-patient interaction spontaneously just because there is a device recording your voices.” According to Calabrese, there is a perception that younger physicians will be more adaptable to the new technology. However, he suggested that practitioners of all ages could experience some discomfort in the way