Add topic to email alerts Receive an email when new articles are posted on Please provide your email address to receive an email when new articles are posted on . “ data-action=”subscribe”> Subscribe We were unable to process your request. Please try again later. If you continue to have this issue please contact customerservice@slackinc.com. Back to Healio Key takeaways: Global Fatty Liver Day, an annual public education and awareness campaign, is observed June 11, 2026. A plethora of new and emerging treatments may change the trajectory of care for fatty liver disease. When Jerry Rosenberg boarded a cruise to Bermuda in April 2017, he was not expecting to return to the U.S. in an air ambulance a few days later. He spent the rest of the month in an induced coma before receiving a liver transplant. Unaware he had metabolic dysfunction-associated steatotic liver disease, an acute episode of hepatitis A — brought about by eating contaminated food — left Rosenberg in critical condition. Jerry Rosenberg “When I was very young, I’d had the [HAV] vaccine, but it was an old vaccine that should have been redone,” Rosenberg told Healio. Rosenberg is not alone. An estimated 1.3 billion people worldwide live with MASLD, according to a global health study in The Lancet Gastroenterology & Hepatology. The road to recovery was not easy. Rosenberg went through transplant rejection twice within 2 years and was prescribed heavy doses of steroids. During this period, Rosenberg became concerned with his weight gain and increased appetite. He reached out to Andrew P. Keaveny, MD, his transplant hepatologist at Mayo Clinic. “Weight gain is very common posttransplant,” Keaveny said. “Patients can experience recurrent fatty liver or develop fatty liver in their new liver.” Initially, Keaveny recommended Rosenberg start taking Mounjaro (tirzepatide, Eli Lilly & Co.), a dual glucose-dependent insulinotropic polypeptide/GLP-1 receptor agonist prescribed off-label for weight loss, but it was not covered by Rosenberg’s insurance. Instead, he began Ozempic (semaglutide, Novo Nordisk), which was. “When I had my once-a-year major checkup on the 9th anniversary of my liver transplant, I was given the news that after 3 years on Ozempic and trying to eat better, I have 0% fat on my liver,” Rosenberg said. Keaveny told Healio that while the dangers of fatty liver disease were appreciated from a hepatology perspective, there were not many treatment options available until recently. “That’s why it’s important to get the message out to [clinicians] to assess patients for fatty liver disease,” Keaveny said. “Previously the pushback was, what can you do about it? Everybody tries to lose weight and they’re not successful. But I think we’ve had a sea change in our approach to identifying and managing MASLD.” Rosenberg is now an advocate for organ donation and patients with fatty liver disease. Healio spoke with Rosenberg and Keaveny in recognition of Global Fatty Liver Day, an awareness campaign recognized annually on the second Thursday of June. Future of care There is an increasing burden of fatty liver disease among younger patients, especially younger males, Keaveny said, citing recent research. It will be important to determine the predominant factors contributing to the condition in this population and others, according to Keaveny. “We need to do more studies to better understand what the dominant player is from an epidemiologic point of view,” Keaveny said. “What are the interactions between disordered metabolism and alcohol.” Emerging therapies, like fibroblast growth factor 21 (FGF-21) analogues, may help alleviate the burden of fatty liver disease by regulating key metabolic pathways to reverse liver fibrosis. Several FGF-21 analogues are now in phase 3 study, including efimosfermin (GSK). “These are very promising as antifibrotic medications, even in patients who have very advanced disease,” Keaveny said. “Currently the treatments that are approved, both resmetirom (Rezdiffra, Madrigal Pharmaceuticals) and Wegovy (semaglutide, Novo Nordisk), are approved for patients who have moderate to severe disease, but not established cirrhosis.” “In the future, there will be multiple medications available, so figuring out sequential therapy and combination therapy is going to be very important, but I think we’re going to have compounds able to address the underlying fibrotic process,” he added. Keaveny also highlighted the significance of preventative medicine in tackling fatty liver disease, especially in light of Rosenberg’s case. “I recommend vaccination against HAV and hepatitis B to all my patients with any form of fatty liver disease, but HAV especially, because that’s one you can just pick up from contaminated food,” Keaveny said. Keaveny is optimistic that these new treatments will reduce the need for liver transplant. “Success in hepatology is reducing the number of patients who need liver transplantations, because if you look at the status of the epidemiology, we’re not going to be able to meet the demand for organs for patients with complications from this condition,” he said. A message for clinicians Screening patients for fatty liver disease — particularly those with type 2 diabetes or a family history of liver disease — is crucial, according to Keaveny. When a patient is diagnosed with fatty liver disease, it is also important to address comorbidities that may be present, he emphasized. “Mild fatty liver disease is a marker of metabolic stress, so it’s very important that individuals with the condition be counseled about their blood pressure, blood sugar and weight as well, to address cardiovascular risk factors,” Keaveny said. Clinicians can connect patients with internet resources to learn more about lifestyle interventions to address fatty liver disease. Keaveny recommends online patient education materials from the American Diabetic Association, American Liver Foundation and Mayo Clinic. He also recommends that clinicians connect patients with dietitians. “Behaviors change gradually, and ongoing support, encouragement and feedback are critical,” Keaveny said. Rosenberg highlighted the “beauty” of support groups for patients. After his transplant, Rosenberg became a member of Mayo Clinic’s Second Chance support group for individuals who have had liver, kidney or pancreas transplantation. “Those of us that have had successful

Menopause Belly – HealthyWomen
I’m standing in front of the mirror squeezing myself into pants that no longer button. I turn to the side and notice soft, squishy love handles, a new belly pooch and skinny legs. Who is this person staring back at me? I go to the gym at least three times a week, I stick to a mostly Mediterranean diet, and I walk everywhere. Why was I suddenly packing on the pounds? And where did these chicken legs come from? As a middle-aged woman in menopause, I knew wrinkles were inevitable. I was prepared for the brain fog and hot flashes, but the weight gain around my abdomen? No one had warned me. I tried to muster up some self-confidence about my body, but I couldn’t find any. Maybe it was hiding underneath all that new belly fat. I did what any other Gen X woman would do and turned to the internet for answers. On TikTok, one chiropractor blamed miscarriages for belly fat, a fitness guru suggested doing endless crunches on Instagram. A doctor on FB swore magnesium was the answer to my woes. Soon my feeds were inundated with ads for supplements and hacks. There was so much conflicting information, I didn’t know who or what to believe. So I signed off of social media and looked into scientific studies. I found out that gaining visceral fat in menopause is pretty common. According to the SWAN study, the majority of women in midlife gain between 4 and 5 pounds over a three-year period. Curious to find out more, I reached out to the experts to learn why this happens and what, if anything, I could do to slow my belly roll. Where does menopause belly fat come from? “Menopause belly is driven by estrogen decline and rising follicle-stimulating hormone (FSH),” said Sara Szal M.D., OB-GYN and author of Women, Food, and Hormones. When your estrogen drops during menopause, you begin to lose muscle mass and gain fat. This creates subcutaneous fat — the soft jiggly muffin top just below your skin. It also creates visceral fat — deeper fat that surrounds your internal organs including the liver, stomach and intestines. Along with drops in estrogen, high levels of FSH — a reproductive hormone — increase fat storage and slow metabolism. This makes it much more difficult to lose weight in midlife. As estrogen continues to drop, your fat gets redistributed from other parts of your body and settles in your belly. A meta-analysis of over 1 million women found that waist circumference increased by 4.6 cm and trunk fat rose by 5.5%, while leg fat significantly decreased by 3.2%. “That’s why the legs look thinner as the midsection grows,” said Salz. This explained my chicken legs. But that’s only part of the story. According to menopause expert Mary Claire Haver, M.D., when you don’t get enough sleep during menopause (and who is?), ghrelin, your hunger hormone, increases. Declining estrogen also reduces leptin, the hormone that tells you when you’re full. So not only are you hungrier, but your body doesn’t signal when you’ve eaten enough. Stress is another culprit. Salz said that chronic stress elevates the stress hormone cortisol, which contributes to visceral fat, insulin resistance and metabolic syndrome. When you’re stressed, you’re also more likely to make poor meal choices or snack on sugary foods. This all leads to inflammation in your body. Inflammation contributes to even more belly fat, brain fog and muscle pain. And this is not simply a vanity concern. It’s not just that we gain a few pounds or go up a few pant sizes. “Visceral fat is dangerous fat,” said Salz. It can increase the risk of breast cancer, dementia, diabetes, heart disease and even sudden death. How to get rid of menopause belly Luckily, there are steps you can take to shrink your menopause belly. Forget the hacks you see online, and follow these well-researched guidelines from Salz and Haver. Follow a Mediterranean diet Why it works: A Mediterranean diet rich in fruits and vegetables, whole grains, nuts, fish and olive oil helps reduce weight and inflammation. Eat protein Why it works: Protein preserves muscle, improves bone density and helps satisfy your hunger. Aim for 30 grams of protein per meal. Add fiber to your diet Why it works: Fiber is the hidden super power for menopause belly. It improves insulin sensitivity, reduces inflammation and helps control your appetite. Aim for 25-40 grams per day from plant-based whole foods, including berries, beans, whole grain oats and legumes. Avoid sugar Why it works: Sugar causes inflammation and contributes to the storage of visceral fat. Aim for less than 25 grams of added sugar per day. Exercise Why it works: Salz said combining high-intensity interval training (HIIT) with resistance training is the most effective way to improve body composition in postmenopausal women. You need a minimum of 150 minutes per week of moderate-intensity aerobic activity and twice weekly muscle-strengthening activities. Lower stress Why it works: Reducing stress lowers your cortisol levels. Make sleep a priority, drink less alcohol–it can spike your cortisol and mess with your sleep–, and consider cognitive behavioral therapy. Journaling, meditation, yoga and breathing exercises can also help. Look into hormone therapy Why it works: Hormone therapy (HT) increases estrogen levels in your body, which helps redistribute visceral belly fat. HT also can improve vasomotor symptoms of menopause (hot flashes and night sweats), sleep quality and your mood, all of which might help you have more energy to exercise consistently. Debunking the myths Now that we know what causes menopause belly, and what we can do about it, let’s hear what Salz said about these menopause belly myths. Myth 1: Crunches and ab workouts reduce belly fat. You cannot spot reduce. No amount of abdominal work will burn fat. Myth 2: Eat less, cardio more and your belly will come off. Aggressive caloric restriction in midlife strips lean mass and worsens the underlying problem. Myth 3: Hormone therapy makes you
Sugar-sweetened beverages linked to hepatocellular carcinoma
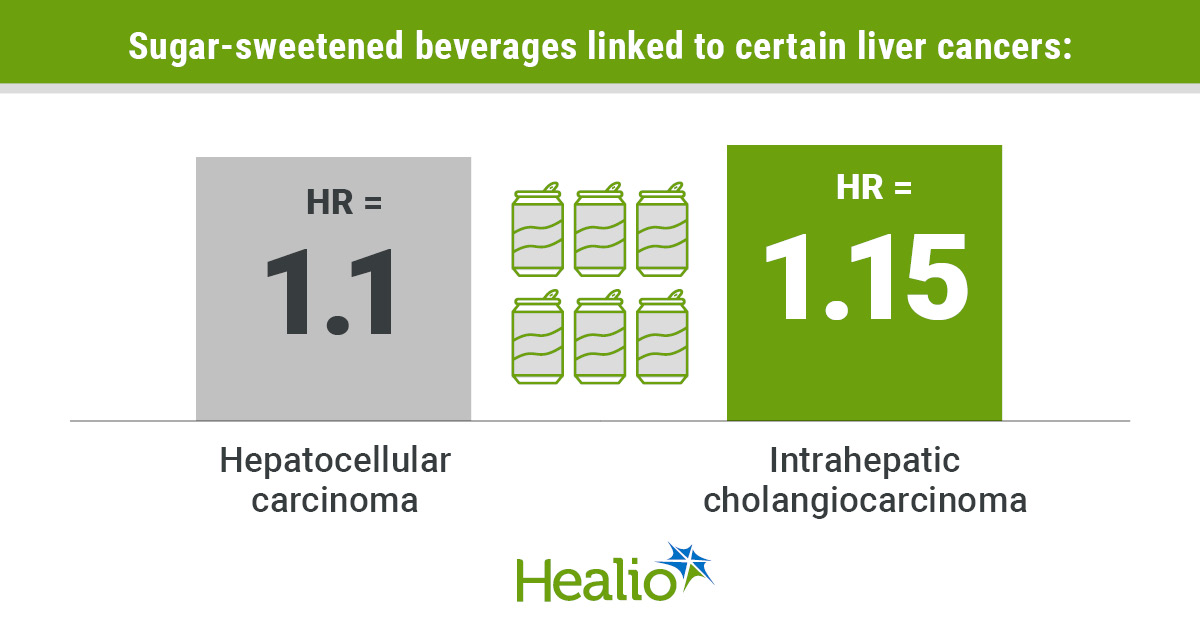
Add topic to email alerts Receive an email when new articles are posted on Please provide your email address to receive an email when new articles are posted on . “ data-action=”subscribe”> Subscribe We were unable to process your request. Please try again later. If you continue to have this issue please contact customerservice@slackinc.com. Back to Healio Key takeaways: Individuals who drank one sugar-sweetened beverage per day had increased risk for hepatocellular carcinoma and intrahepatic cholangiocarcinoma. Artificially sweetened beverages did not increase risk. Consuming sugar-sweetened beverages may significantly increase the risk for specific types of liver cancer. A pooled analysis including more than a million individuals found those who drank one sugar-sweetened beverage per day had a 10% greater risk for hepatocellular carcinoma and 15% greater risk for intrahepatic cholangiocarcinoma (ICC). Data derived from Watling CZ, et al. JAMA Netw Open. 2026;doi:10.1001/jamanetworkopen.2026.17754. Artificially sweetened beverages did not significantly increase the risk for any form of liver cancer. “The overall evidence for an association in humans between artificially sweetened beverages and liver cancer, and more specifically aspartame and HCC, is not strongly supported by these analyses,” Cody Z. Watling, DPhil, postdoctoral fellow in the division of cancer epidemiology and genetics at NCI, and colleagues wrote. “Based on this study and prior research associating sugar-sweetened beverages with adverse outcomes, individuals may benefit from reducing their intake of sugar-sweetened beverages.” Unknown risk factor? Global liver cancer diagnoses are projected to increase 55% by 2040, according to study background. In the U.S., more than 42,000 individuals are expected to be diagnosed in 2026, and nearly 31,000 will die from the disease, according to American Cancer Society’s Cancer Statistics 2026 report. Common risk factors for HCC, the most diagnosed form of the disease, include chronic hepatitis B or C virus infection, excessive alcohol use, smoking, metabolic dysfunction-associated steatotic liver disease (MASLD), obesity and diabetes. “However, an estimated 35% of HCC cases are not explained by known risk factors,” researchers wrote. Prior studies have produced mixed results on the potential association between aspartame, an artificial sweetener, and liver cancer. Previous research has associated sugar-sweetened beverages with multiple risk factors for liver cancer, including diabetes, MASLD and weight gain, but prospective studies have been limited in investigating the link to the malignancy itself. “We aimed to investigate associations between intake of artificially sweetened beverages and sugar-sweetened beverages and risk of total liver cancer, HCC and ICC,” researchers wrote. The pooled analysis of 11 prospective cohort studies included 1,518,411 participants (mean age, 57.8 years; standard deviation, 10.1; 58.2% women; mean BMI, 26.5 kg/m2, standard deviation, 5) who had no history of cancer. Enrollment across cohorts stretched from 1980 to 2009, and the overall study population had a median follow-up of 17.8 years. Participants self-reported intake of artificially sweetened and sugar-sweetened beverages. Incident liver cancer, HCC and ICC served as the primary endpoint. ‘The largest study’ Researchers did not observe a significant association with artificially sweetened beverages and liver cancer, HCC or ICC. “In models not adjusted for diabetes or BMI, we observed positive associations between artificially sweetened beverage consumption and liver cancer risk, but after adjustment for these confounders was made, outcomes were attenuated and there were no longer associations,” researchers wrote. “In most cohorts, participants who consumed one or more artificially sweetened beverages per day were more likely to have been diagnosed with diabetes and have a higher BMI at baseline than individuals who never or rarely consumed artificially sweetened beverages.” Watling and colleagues did find sugar-sweetened beverages had a significant association with both HCC (HR per 1 drink/day intake = 1.1; 95% CI, 1.03-1.18) and ICC (HR per 1 beverage/day intake = 1.15; 95% CI, 1-1.32), but not overall liver cancer. Individuals with baseline diabetes had similar risks for liver cancer regardless of their consumption of artificially sweetened and sugar-sweetened beverages. “It remains unclear whether increased consumption of sugar-sweetened beverages contributes to increased risk of HCC independent of obesity and diabetes,” researchers wrote. Watling and colleagues acknowledged study limitations, including self-reported consumption of artificially sweetened and sugar-sweetened beverages, and inability to stratify for underlying liver disease, including MASLD. “To our knowledge, this is the largest study to date to assess the association of artificially sweetened beverage and sugar-sweetened beverage intake with liver cancer risk,” they wrote. Perspective Back to Top The results were not particularly surprising, striking or unexpected, though they were drawn from a very thorough pooled analysis of studies with extended follow-up. This pooled analysis confirmed a very mild increased risk for liver cancer associated with sugar-sweetened beverages, but it did not demonstrate a significantly increased or reduced risk for liver cancer associated with the consumption of artificially sweetened beverages. It is difficult to determine if the risk associated with sugar-sweetened beverages is truly causal in nature or not. Given that these beverages have little to no nutritional value beyond the sugar itself, it may be wise to limit consumption. Importantly, the risks are not nearly as striking as those of other well-established risk factors for liver cancer, including liver cirrhosis or chronic infection with viral hepatitis B or C. Vaccination for hepatitis B, screening/treatment of hepatitis C, and avoiding exposure to known liver toxins, such as alcohol or aflatoxins, remain the bedrock recommendations for liver cancer prevention. It will be important to continue to investigate the possible associations between consumption of these beverages and other cancers or health hazards. Ernest Hawk, MD, MPH The University of Texas MD Anderson Cancer Center Disclosures: Hawk reports no relevant financial disclosures. Published by: Sources/Disclosures Source: Watling CZ, et al. JAMA Netw Open. 2026;doi:10.1001/jamanetworkopen.2026.17754. Reference: Disclosures: Watling reports no relevant financial disclosures. Please see the study for all other authors’ relevant financial disclosures. Ask a clinical question and tap into Healio AI’s knowledge base. PubMed, enrolling/recruiting trials, guidelines Clinical Guidance, Healio CME, FDA news Healio’s exclusive daily news coverage of clinical data Learn more

Información comprobada sobre la vacuna contra el VRS
English El virus respiratorio sincitial (VRS) es una infección frecuente que ataca los pulmones y el sistema respiratorio. Es tan frecuente que muchos niños se infectan con el virus antes de su segundo cumpleaños. Pero el VRS no solo enferma a los niños, este virus también puede infectar a adultos. El VRS afecta la mucosa de las vías respiratorias y cuando el sistema inmunitario lanza un ataque, eso causa inflamación y una producción excesiva de mucosidad. Las vías respiratorias se estrechan y se obstruyen con mucosidad, residuos celulares y líquidos, lo que puede dar la sensación de soplar por un sorbete de plástico o de silbar por un acordeón desinflado cuando se trata de respirar. Si bien muchas infecciones son leves, bebés de menos de 2 meses, todos los adultos de más de 75 años y adultos de más de 50 años con trastornos crónicos tienen un mayor riesgo de infecciones graves y hospitalizaciones. ¿Cómo se disemina el VRS? El VRS es contagioso y se propaga como la gripe. Tos y estornudos expulsan microgotas diminutas al aire y a superficies. Puedes contagiarte del virus si respiras estas microgotas o si llegan a tus ojos, nariz o boca porque alguien tose o estornuda cerca de ti o si tocas una superficie contaminada y luego tocas tu rostro antes de lavar tus manos. Lee: ¿Es covid, el VRS o gripe? >> ¿Quién debería vacunarse en contra del VRS? En EE.UU., los Centros para el control y prevención de enfermedades (CDC, por sus siglas en inglés) recomiendan una vacuna contra el VRS para adultos de 75 años o más o para adultos de más de 50 años con trastornos que les dan un mayor riesgo de enfermarse gravemente con VRS y de hospitalizaciones. ¿Qué trastornos incrementan el riesgo de enfermarse gravemente con VRS? El VRS puede ser duro para personas con órganos deteriorados o con sistemas inmunitarios débiles. Algunos trastornos te dan un mayor riesgo de enfermarte gravemente con este virus. Estos trastornos son, entre otros: EPOC Insuficiencia cardiaca congestiva Diabetes Enfermedades hepáticas crónicas Obesidad Habla con tu proveedor de atención médica (HCP, por sus siglas en inglés) si no conoces con certeza tu riesgo. ¿Con qué frecuencia debes vacunarte contra el VRS? Actualmente, los CDC recomiendan solo una vacuna contra el VRS para adultos de más de 75 años o para adultos de 50 a 74 años que tienen mayor riesgo de enfermarse gravemente con el VRS. Deberías recibir esta vacuna incluso si la recibiste durante el embarazo. ¿Cuál es el mejor momento para vacunarse contra el VRS? La temporada del VRS generalmente es de octubre a marzo, aunque eso puede variar dependiendo de la parte del país en que vives. El mejor momento para vacunarse es durante los últimos meses del verano o durante los primeros meses del otoño antes de que empiece la temporada de VRS, pero puedes vacunarte en cualquier momento. Pregunta a tu proveedor de atención médica en qué momento te recomienda que te vacunes en tu área. ¿Cuáles son los efectos colaterales de la vacuna contra el VRS? Las vacunas contra el VRS tienen efectos colaterales parecidos a los de otras vacunas, los cuales usualmente son leves, y podrían ser, entre otros: Dolor en el lugar de la inyección Fatiga Fiebre Dolor de cabeza Náuseas Dolor articular o muscular ¿Cuáles son los beneficios de la vacuna contra el VRS? Los beneficios de vacunarse superan inmensamente los riesgos. Vacunarse contra el VRS es el mejor método para prevenir enfermedades graves y complicaciones tales como eventos cardiacos desencadenados por la inflamación causada por el virus. También reduce sustancialmente las tasas de hospitalización causadas por el VRS para adultos mayores. Y un estudio incluso indica que vacunarse contra el VRS puede reducir el riesgo de demencia en etapas posteriores de la vida. Los beneficios de vacunarse contra el VRS son similares para personas embarazadas, previniendo hospitalizaciones y enfermedades graves. También proporciona protección al feto cuando la vacuna se aplica entre la semana 32 y 36 del embarazo. La vacunación durante el embarazo ha demostrado una reducción del 68% de hospitalizaciones para recién nacidos que se contagian del VRS. Si una mujer no se vacuna durante el embarazo, su bebé puede recibir una inyección para bebés de anticuerpos contra el VRS de acción prolongada después del nacimiento para evitar hospitalizaciones y enfermedades graves. Además de los beneficios médicos, vacunarte puede ayudar a tu comunidad. Sí comunidades tienen buenos niveles de vacunación, los adultos pierden menos días de trabajo, los estudiantes pierden menos días de escuela y los hospitales tienen menos carga por brotes de enfermedades. Este recurso educativo se preparó con el apoyo de Moderna. From Your Site Articles Related Articles Around the Web Source link
Author Lindsay Hameroff on ‘Rewrite the Stars’ & Autism Representation
If you purchase an independently reviewed product or service through a link on our website, SheKnows may receive an affiliate commission. This isn’t the first time Lindsay Hameroff considered writing a character with autism. Hameroff has two children on the spectrum, and she was midway through her first book when her youngest was diagnosed. She thought about how she might include a side character with autism, mapping out where he might slot into the story, before realizing it wasn’t the right fit. “[My review group] told me, ‘You don’t want to take that opportunity and make it feel tokenized,’” she tells SheKnows. So, Hameroff waited until the time was right — and now, she says she’s glad she did. In Rewrite the Stars, out July 7, Marissa Morgan is a divorced Hollywood starlet and mom to two kids, one of whom has autism. When Marissa’s famous ex-husband gets back together with his famous first wife (yes, the Ben-Jen-Jen love triangle was the inspiration), she decamps to the Pocono Mountains with her kids, craving an escape from the media circus. Related story The Brand Famous for Designer Fashion Dupes Makes the Best Greens Powder—So You Can Stop Overpaying for Yours The novel centers on the sweet romance between Marissa and Jesse, the childhood friend-turned-carpenter working on her house, but Marissa’s role as a mom is what sets everything in motion. As her ex reunites with his old flame and the paparazzi swarm Marissa’s house, “she is very stressed out about the impact it’s going to have on her children,” Hameroff explains. That anxiety is what prompts her to leave Hollywood for Pennsylvania. “What sets the novel into motion,” Hameroff says, “is a decision she makes for the welfare of her kids.” It was Hameroff’s first time writing from the perspective of a mother, but she says it felt natural. Writing Levi, Marissa’s autistic child, though, came with some nerves. “The representation needs to feel right,” she remembers thinking. “It needs to feel authentic.” Rewrite the Stars: A Novel Hameroff drew heavily from her own parenting experience. She also got inspiration from bestselling author Kennedy Ryan, whose novel This Could Be Us includes a character whose son has autism. Hameroff picked Ryan’s brain about writing a neurodivergent caregiver and “she sort of gave me the confidence to go for it,” Hameroff says. But Ryan also advised her that “people are very sensitive about certain aspects of autism,” Hameroff recalls. “So, I was very nervous about it.” There are many aspects that feel true to life about Levi’s character — because they are. Hameroff’s son, for example, once went through a phase of only eating miniature Eggo waffles, a detail Hameroff borrowed for Levi. “Autism is a spectrum,” Hameroff notes. “It’s going to be different for everybody, but this is one snapshot of one lived experience.” Other details are pulled from real life, too. When Marissa talks about Levi’s diagnosis with other parents, their responses echoed real conversations Hameroff had. “People meant well, but they said things that felt like a gut punch,” Hameroff recalled, like, “‘This is every parent’s nightmare. We’re so sorry this is happening to you.’” The true-to-life details and emotions made Rewrite the Stars the most difficult book Hameroff has written. Some days, she says, working on the book felt like pulling teeth because it was so close to to her heart. The pressure of representation was also heavy. “Writing this book was very therapeutic,” Hameroff says, “but at the same time, knowing that I was writing about something that people were going to relate to — being a single mom, a divorced mom, and a caregiver for children and children on the spectrum — I felt a responsibility to really get it right.” The early reviews are trending in that direction. “The feedback I’ve gotten about the representation and parenting has been, ‘I feel seen, and I relate to this,’” Hameroff says, “and that is exactly what my goal was for this book. I wanted to write a love letter to other moms.” Source link
Effective Cell Therapy for Hair Regeneration
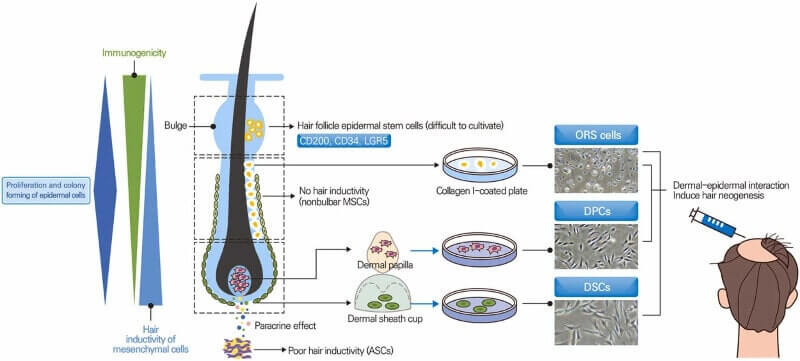
Update: June 8, 2026 More new Papers from Jong-Hyuk Sung Epibiotech’s CEO and prolific hair loss researcher Jong-Hyuk Sung has co-authored two new major papers in recent months: Update: Epibiotech CEO Sung (who is the author of the new 2022 paper covered in this post) is answering our questions in the comments this week. Please note that English is not his first language. Q & A has now ended. November 25, 2022 Effective cell Therapy for Hair Regeneration Earlier this month, Epibiotech CEO Jong-Hyuk Sung published a detailed new paper titled “Effective and economical cell therapy for hair regeneration.” It was widely covered in South Korean media (h/t “Theo”, who also sent me this update on Mr. Sung’s presentation covering the paper). They call him Seong Jong-Hyeok in that article. My interest piqued when I read such a thorough scientific paper from a CEO. Almost unheard of in the western world. I showed it to a well known US hair transplant doctor, and he found it to be a great summary. Adipose-Derived Stem Cells, Dermal Papilla Cells and Dermal Sheath Cup Cells Note that Dr. Sung has published numerous papers on adipose-derived stem cells and hair regeneration (and wound healing) for 15 years. This CEO seems to be a scientist first and foremost, rather than a business person. This latest paper covers the three main types of cell based hair regeneration treatment strategies that are currently being developed: Adipose-derived stem cells (ADSC or ASC). Dermal papilla cells (DPC). Dermal papilla epithelial cup cells, better known as dermal sheath cup cells (DPSC or DSC). The paper also mentions the manufacturing of hair organoids using induced pluripotent stem cells. Including a shout out to Dr. Takashi Tsuji. Note that Shiseido (including its use of Replicel’s technology) now offers a hair regeneration treatment involving culturing of dermal sheath cup cells. Also note that in the past, Aderans and Intercytex both saw some success in hair growth via dermal papilla cell culturing and injection into balding scalps. HairClone is currently trying something similar. Dr. Sung’s company Epibiotech is ultimately driven by “Off-the-shelf” allogeneic DPC therapy. It aims to begin Phase 1 clinical trials for its EPI-001 dermal papilla cell hair multiplication treatment in 2023. We are all hopeful that things will move faster in Asia in comparison to the US or Western Europe. The company can already mass-produce dermal papilla cells with hair growth ability using spheroid culture, hypoxic conditions, and growth factors. Cell therapy for hair growth. Adipose, dermal papilla and dermal sheath cup cells. Source: Biomedicine & Pharmacotherapy, January 2023. Adipose Derived Stem Cells Given the author’s background, the paper is especially detailed when it comes to ADSC (ASC). Dr. Sung highlights the pros and cons. Adipose-derived stem cells are easy to access and isolate in large quantities. This is not true when it comes to dermal papilla cells and dermal sheath cup cells. While ASCs promote hair growth through the paracrine effect, they have a poor potential in hair neogenesis. Dr. Sung suggests further development in methods to enhance the trichogenecity of ASCs. Other New Recent Studies on Hair Regeneration As if this was not enough, two new papers on hair regeneration came out in the past month. A literature review from Japan covers numerous cell therapies for hair regrowth. This includes mesenchymal stem cell (MSC) implantation. Adult sources of MSC include: adipose tissue (including SVF); bone marrow; DPC; DSC; placenta and umbilical cord. The paper also analyzes non-cell therapies, including exosomes, extracellular matrix, platelet-rich plasma, and the MSC secretome. The last mentioned “comprises bioactive materials, such as growth factors, cytokines and nucleic acids that play an important role in regulating the hair follicle cycle and regeneration”. A new study from China on microenvironmental reprogramming of human dermal papilla cells for hair follicle tissue engineering. Source link
Judge overturns H-1B visa fee barrier to foreign-born physicians
Add topic to email alerts Receive an email when new articles are posted on Please provide your email address to receive an email when new articles are posted on . “ data-action=”subscribe”> Subscribe We were unable to process your request. Please try again later. If you continue to have this issue please contact customerservice@slackinc.com. Back to Healio Key takeaways: A U.S. district judge voided an H-1B visa fee instituted in the fall. The fee would negatively affect the U.S. physician workforce, labor groups said. A bill before Congress would exempt health care workers. A federal judge voided a policy instituted by presidential proclamation last fall that raised the application fee for new H-1B visas to $100,000. As Healio previously reported, the H-1B visa program allows employers to temporarily hire foreign workers in certain occupations that require specialized knowledge, including certain international medical graduates. Nearly 250,000 international medical graduates worked in the United States in 2023, making up 24.7% of the total U.S. physician workforce. The fee increase was predicted to have large and lasting negative effects on the U.S. physician workforce, according to the AMA and medical specialty groups. In summary judgment in California v. Mullin, the judge ruled the fee increase violated the Administrative Procedure Act by imposing a tax that can be authorized only by Congress. The suit was brought in the U.S. District Court for the District of Massachusetts, but because the ruling was based on federal law, it applies nationwide, according to Linda Gemind, an immigration attorney at Benesch in Cleveland. “Although it’s likely not the end of the matter, the ruling should take us back to pre-implementation of the $100,000 fee — for now,” Gemind told Healio. “At this point it should be the standard fee, which is generally $3,380 ($780 filing fee, $1,500 [American Competitiveness and Workforce Improvement Act] fee, $500 fraud fee, $600 asylum fee) for most petitions.” The AMA praised the ruling. “Today’s decision blocking the $100,000 visa fee is a victory for patients,” AMA President Bobby Mukkamala, MD, said in a press release. “At a time when communities across the country face physician shortages and growing barriers to care, we should be removing obstacles — not creating new ones — to attract talented physicians and other highly skilled professionals. International medical graduates play a vital role in caring for patients, particularly in underserved and rural areas.” The Trump administration will likely appeal the ruling in the U.S. Court of Appeals for the First Circuit or the U.S. Supreme Court, if it can establish jurisdiction, Gemind said. A judge could stay the decision until after the appeals process, but that has not happened so far. If the ruling ultimately stands, employers who have already paid the increased fee will likely seek refunds and those who chose not to apply for a visa because of the fee will also likely litigate, according to Gemind. In addition to legal challenges to the fee increase, a bipartisan group introduced a bill — H.R. 7961 — in the U.S. House of Representatives in March, which would exempt health care workers. For more information: Linda Gemind can be reached at lgemind@beneschlaw.com. Published by: Sources/Disclosures Source: Healio Interviews References: AAMC U.S. Physician Workforce Data Dashboard. https://www.aamc.org/data-reports/report/us-physician-workforce-data-dashboard. Accessed June 10, 2026. AMA applauds court decision blocking $100,000 visa fee for physicians. https://www.ama-assn.org/press-center/ama-press-releases/ama-applauds-court-decision-blocking-100000-visa-fee-physicians. Published June 8, 2026. Accessed June 9, 2026. H. R. 7961. https://www.congress.gov/119/bills/hr7961/BILLS-119hr7961ih.pdf. Published March 17, 2026. Accessed June 10, 2026. National Center for Health Workforce Analysis. Physician Workforce: Projections, 2023-2038. https://bhw.hrsa.gov/sites/default/files/bureau-health-workforce/data-research/physicians-projections-factsheet.pdf. Published December 2025. Accessed June 10, 2026. Memorandum and order on plaintiffs’ motion for summary judgment (doc. no. 86) and defendants’ cross-motion for summary judgment and motion to dismiss (doc. no. 92). https://storage.courtlistener.com/recap/gov.uscourts.mad.293201/gov.uscourts.mad.293201.106.0.pdf. Published June 8, 2026. Accessed June 9, 2026. Disclosures: Gemind reports no relevant financial disclosures. Ask a clinical question and tap into Healio AI’s knowledge base. PubMed, enrolling/recruiting trials, guidelines Clinical Guidance, Healio CME, FDA news Healio’s exclusive daily news coverage of clinical data Learn more Add topic to email alerts Receive an email when new articles are posted on Please provide your email address to receive an email when new articles are posted on . “ data-action=”subscribe”> Subscribe We were unable to process your request. Please try again later. If you continue to have this issue please contact customerservice@slackinc.com. Back to Healio Source link
Facts About the RSV Vaccine
Español Respiratory syncytial virus (RSV) is a common infection that targets the lungs and respiratory system. It’s so common that many children have been infected with the virus before their second birthday. But RSV doesn’t just make children sick, the virus can also infect adults. RSV disrupts cell linings in the respiratory tract and when the immune system launches an attack, it stirs up inflammation and an overproduction of mucus. Airways become narrow and clogged with mucus, cell debris and fluid, which can make breathing feel like blowing through a plastic straw or wheezing like a deflated accordion. While many infections are mild, infants under 2 months, all adults over age 75 and adults over 50 with chronic conditions are at higher risk for serious infections and hospitalizations. How does RSV spread? RSV is contagious and spreads like the flu. Coughing and sneezing blast tiny microdroplets into the air and onto surfaces. You can get the virus when you breathe in these microdroplets or they get into your eyes, nose or mouth because someone coughs and sneezes near you, or you touch a contaminated surface and then touch your face before washing your hands. Read: Is It Covid, RSV or the Flu? >> Who should get the RSV vaccine? In the U.S., the Centers for Disease Control and Prevention (CDC) recommends an RSV vaccine for any adult 75 and older, or those over 50 with conditions that put them at higher risk for severe RSV disease that can lead to hospitalizations. What conditions increase the risk of severe illness from RSV? The RSV virus can be ruthless in people with impaired organ function or compromised immune systems. Several conditions put you at high risk for getting severely ill from the virus. These conditions include: Check with your healthcare provider (HCP) if you’re uncertain about your risk status. How often do you need a RSV vaccine? Currently, the CDC recommends just one RSV vaccine as an adult over age 75 or an adult ages 50-74 who is at increased risk of severe illness from RSV. You should receive this vaccine even if you received it while pregnant. When is the best time to get an RSV vaccine? RSV season is generally October through March, although that can vary depending on what part of the country you live in. The best time to get vaccinated is late summer or early fall before RSV season starts, but you can get vaccinated at any time. Ask your HCP when they recommend getting the shot in your area. What are the RSV vaccine side effects? RSV vaccines have similar side effects as other vaccines, which are usually mild, and can include: Pain at the injection site Fatigue Fever Headache Nausea Joint or muscle pain What are the benefits of the RSV vaccine? The benefits of getting vaccinated far outweigh the risks. Getting the RSV vaccine is the best way to prevent serious illness and complications from serious illness, like a cardiac event triggered by inflammation from the virus. It also substantially reduces hospitalization rates for RSV in older adults. And one study even indicated that getting the RSV vaccine can lower the risk of dementia later in life. The benefits of getting the RSV vaccine are similar for pregnant people — preventing serious illness and hospitalization. It also provides protection to the fetus when the vaccine is given sometime between 32 to 36 weeks of pregnancy. Maternal vaccination has shown a 68% reduction in infant hospitalization in newborns who get RSV. If a woman didn’t receive the vaccine while pregnant, her infant can get a long-acting infant RSV antibody injection after they’re born to protect them from developing severe disease and keep them out of the hospital. In addition to health benefits, getting vaccinated can help your community. When populations are well vaccinated, adults miss less work, students miss less school, and hospitals are less stressed by disease outbreaks. This educational resource was created with support from Moderna. From Your Site Articles Related Articles Around the Web Source link

Laser Cap vs Medical-Grade LLLT for Hair Loss: What Works?
If you’ve been searching for at-home laser caps, you’re not alone. At-home devices have become one of the most talked-about options for treating hair thinning. They’re convenient, easy to use, and promise visible results. But how do they actually compare to in-clinic treatments like medical-grade LLLT? And more importantly, which one is worth it? At NHLMA in Scottsdale, we are big advocates of LLLT at the highest medical-grade form because our patients have seen great success from it. What is LLLT for hair loss? LLLT hair loss treatment uses low-level light to stimulate the scalp and support healthier hair growth. It works by: increasing blood flow to the follicles extending the hair growth cycle supporting thicker, stronger strands over time It’s non-invasive and widely used for early to moderate hair thinning. Source link
Study: Moxifloxacin bests azithromycin in treating M . gen italium
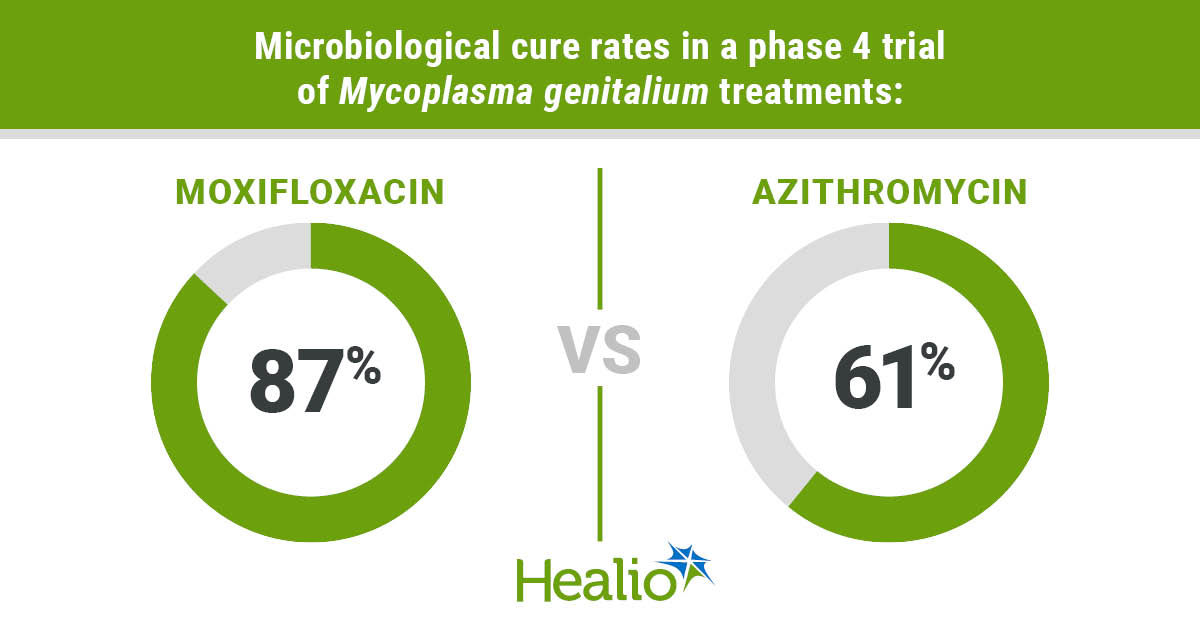
Add topic to email alerts Receive an email when new articles are posted on Please provide your email address to receive an email when new articles are posted on . “ data-action=”subscribe”> Subscribe We were unable to process your request. Please try again later. If you continue to have this issue please contact customerservice@slackinc.com. Back to Healio Key takeaways: A phase 4 trial demonstrated an 87% cure rate for moxifloxacin in treating Mycoplasma genitalium. A researcher said it is “not surprising” moxifloxacin performed better than azithromycin. A study that compared the efficacy of moxifloxacin vs. azithromycin in treating Mycoplasma genitalium — an STI with a rising resistance to antibiotics — showed that moxifloxacin was the clear winner. In the phase 4 randomized trial, a 10-day regimen of moxifloxacin yielded a significantly higher microbiologic cure rate compared with a 6-day regimen of azithromycin (87% vs. 61.2%; absolute risk difference, 25.8%; 95% CI, 16.5%-35.2%), supporting moxifloxacin as an empiric first-line treatment. Data derived from Rossotti R, et al. Clin Infect Dis. 2026;doi:10.1093/cid/ciag317. The study pointed out, however, that azithromycin “showed comparable efficacy” among heterosexual participants. “It is not surprising that moxifloxacin performs better than azithromycin in a population largely composed of” gay, bisexual and other men who have sex with men (MSM), the study’s lead author, Roberto Rossotti, MD, associate professor of infectious diseases at University of Verona in Italy, told Healio. “But it is surprising that this performance is comparable to that observed with the resistance-guided approach, saving 4 days of treatment and one class of antibiotics.” M. genitalium is a common STI that causes a burning while urinating and discharge from the vagina or penis, according to the CDC.eatment has become tricky due to a macrolide resistance to azithromycin, once a first-line treatment, with resistance rising from 10% before 2010 to 51% in 2016-2017, researchers reported. Rossotti and colleagues conducted the trial in a tertiary care hospital located in Milan from January 2018 to June 2024. They randomly assigned 358 patients (median age, 36 years; 96.6% men; 94.1% gay, bisexual and other MSM; 5.9% heterosexual) to moxifloxacin (53.9%; n = 193) or azithromycin (46.1%; n = 165). Moxifloxacin was administered as a once-daily 400 mg dose for 10 days, whereas azithromycin was given as a 500 mg daily dose for 6 days. In addition to the main finding, the study showed a success rate of moxifloxacin in retreatment. Specifically, 96.8% of participants (30 out of 31) who failed an initial round of azithromycin were cured with moxifloxacin, whereas a second round of azithromycin only cured 60% of individuals (nine out of 15; P = .003). The study also found that co-administering doxycycline did not enhance treatment outcomes in either group. “A 10-day course of moxifloxacin may achieve 90% microbiologic success even if a resistance test is not available,” Rossotti said. M. genitalium is a leading cause of non-gonococcal urethritis in men and linked to cervicitis in women, the CDC reported. Meanwhile, Rossotti said the study gives clinicians hope in treating the stubborn infection. “We may be reassured about the everyday clinical management of (M. genitalium) based on a relatively short course of quinolone therapy alone,” he said. For more information: Roberto Rossotti, MD, can be reached at infectiousdisease@healio.com. Perspective Back to Top Management of M. genitalium remains challenging for many reasons, including limited access to macrolide resistance testing despite a high prevalence of resistant infections. The results of this study comparing monotherapy for M. genitalium with azithromycin vs. moxifloxacin illustrate the consequences of this prevalence; rates of azithromycin treatment failure roughly correspond to reported rates of macrolide resistance in Europe. U.S. and U.K. guidelines only recommend azithromycin use when M. genitalium susceptibility is confirmed, and after a preceding week of doxycycline. This strategy enables successful use of azithromycin in M. genitalium treatment while avoiding de novo resistance, and stewards moxifloxacin, currently the only other widely available therapy for this infection in the U.S. Where resistance testing is not available, sequential therapy with doxycycline and moxifloxacin remains the standard for patients who are not pregnant. The utility of doxycycline (and other agents) as a part of moxifloxacin-based M. genitalium regimens merits further study, especially as rates of quinolone resistance rise. The relatively small number of patients receiving doxycycline in this study limits conclusions as to its role (or lack thereof) alongside moxifloxacin. Future efforts to improve M. genitalium therapy need to address access to macrolide (and potentially fluoroquinolone) resistance testing and rigorously compare treatment strategies that minimize antibiotic exposure and steward available agents without sacrificing efficacy. Jacob McLean, DO Adult Infectious Disease Physician and Assistant Professor of Medicine at New York Presbyterian Columbia University Irving Medical Center. Disclosures: McLean reports no relevant financial disclosures. Published by: Ask a clinical question and tap into Healio AI’s knowledge base. PubMed, enrolling/recruiting trials, guidelines Clinical Guidance, Healio CME, FDA news Healio’s exclusive daily news coverage of clinical data Learn more Add topic to email alerts Receive an email when new articles are posted on Please provide your email address to receive an email when new articles are posted on . “ data-action=”subscribe”> Subscribe We were unable to process your request. Please try again later. If you continue to have this issue please contact customerservice@slackinc.com. Back to Healio Source link